Medullary Thyroid Cancer Surgery Basics: From Minimally Invasive Surgery to Comprehensive (Appropriate) Surgery
For medullary thyroid cancer, surgery, by far, is the most common first treatment. In fact, in favorable smaller medullary thyroid cancers, surgery is not only the first treatment but is commonly the only treatment that may be indicated. It is critical that a highly experienced surgeon and the right surgery is obtained the first time. Medullary thyroid cancer surgery should only be done by expert surgeons. By choosing the right surgeon and surgery, you are provide the greatest opportunity for cure and long term control of disease. The wrong choice may lead to repeated surgeries, complications, and even worse! Find out what our medullary thyroid cancer patients say about us on our Google reviews and Health Grade reviews here.
Thyroid surgery was one of the first ever described surgeries in medicine, but early on it wasn't very pretty or safe. Over the past 100 years, thyroid surgery has evolved into its current state of the art by some of the most recognized names in surgical history. Today, in skilled hands, medullary thyroid cancer surgery may be considered an art form in and of itself.
Medullary thyroid cancer surgery must be considered in several different lights when you think about the neck. Surgery of the thyroid gland itself and surgery for the lymph nodes of the neck. The basic concept is however very simple, remove all of the cancer.
The central compartment lymph node surgery spares all critical structures including the nerves to the voice box and all parathyroid glands not directly involved by cancer. Central compartment dissection extends from the carotid arteries on both sides of the neck, below to the blood vessels of the upper chest, and above to where the blood vessel of the upper portion of the thyroid gland begins off of the carotid artery (called the superior thyroid artery). [see a ]
- In medullary thyroid cancer, the central compartment lymph nodes are at risk of containing cancer in up to 70% of patients. That risk increases with the size of the medullary thyroid cancer. Even though the medullary thyroid cancer patient may have no identifiable lymph nodes with cancer on ultrasound or CT scan, complete dissection is indicated due the very high lymph node metastatic rate and recurrence rate without this intervention.
- In medullary thyroid cancer surgery, expert surgeons who perform this surgery routinely are required to remove all the necessary lymphatic areas and involved tissues and spare the nerves to the voice box and the critical glands that control calcium (parathyroid glands).
Extended or Complicated Thyroidectomy
Medullar thyroid cancer may sometimes be more aggressive than ultrasound or CT imaging suggested prior to undergoing surgery. In these cases, an expert surgeon that recognizes those "more aggressive" intraoperative findings such as growth or extension of the cancer outside of the thyroid gland or invasion of the cancer into adjacent structures such as the nerve to the voice box (recurrent laryngeal nerve), breathing tube (trachea), voice box, or esophagus-must adapt the surgery to adequately address the complete removal of the cancer. Unfortunately, occasional thyroid surgeons are commonly unprepared to perform the appropriate surgery and a subsequent surgery for persistent disease will be required ). An incomplete first attempt at surgery greatly increases the risk for local recurrence, complications from subsequent surgeries, and even death from disease.
Medullary Thyroid Cancer Surgery For Spread of Cancer to Lymph Nodes Along The Side Of The Neck (anterolateral neck) =
- Just the presence of enlarged lymph nodes does not mean medullary thyroid cancer has spread and does not require additional surgery
- A procedure called an anterolateral neck dissection (or modified neck dissection), in untreated patients, should only be performed in instances of ultrasound with fine needle aspiration confirmed medullary thyroid cancer spread to lymph nodes in the side of the neck
- The medullary thyroid cancer anterolateral neck dissection is not the same neck dissection as for other cancers that occur in the neck. Medullary thyroid cancer spreads to particular areas of the neck called levels. Removing just some of the lymph nodes has been called "cherry picking" and is the wrong surgery! A medullary thyroid expert surgeon trained and experienced to perform modified neck dissections specifically for thyroid cancer is needed to prevent recurrent or persistent disease.
- The anterolateral neck dissection, in skilled hands, spares all critical nerves, muscles, and blood vessels which are not directly involved with cancer (very rarely are critical structures involved by papillary thyroid cancers). It is an approximately 40 minute surgery that removes lymph nodes and fatty tissue.
- The anterolateral neck dissection should be performed electively on the same side as large medullary thyroid cancer masses when the great vessels of the neck need to be dissected as well.
- Ultrasound and CT scan node negative necks need not be electively dissected with initial surgery for smaller medullary thyroid cancers.
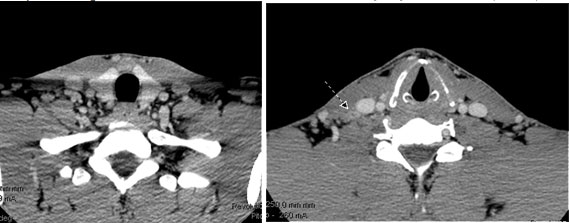 Patient presentation: A 32 year old firefighter, rescue public servant from Georgia presents with a suspicious right lateral neck lymph node. Fine needle biopsy suggests medullary thyroid cancer. He has no known family history of medullary thyroid cancer, adrenal tumors, or sudden cardiac death. Genetic testing reveals this to be a non-hereditary medullary thyroid cancer. His CT scans of his neck below reveal the suspicious right neck mass confirmed to be medullary thyroid cancer (arrow).His CT scan of his chest and neck do not reveal evidence of spread. His calcitonin is 3179 and his CEA is 18.6 before surgery.His surgery includes a total thyroidectomy, central compartment dissection and right anterolateral neck dissection. Right inferior parathyroid gland autotransplanted.
Pathology
Medullary thyroid cancer 1.4 cm
Central compartment dissection 4 of 22 lymph nodes with spread of medullary thyroid cancer
Right anterolateral neck dissection 6 of 36 lymph nodes with spread of medullary thyroid cancer
Three year follow up:
Calcitonin below any detectable levels
CEA 1.6 ng/ml
Ultrasound without any abnormalities
Patient is highly likely cured of his medullary thyroid cancer!!
Patient presentation: A 32 year old firefighter, rescue public servant from Georgia presents with a suspicious right lateral neck lymph node. Fine needle biopsy suggests medullary thyroid cancer. He has no known family history of medullary thyroid cancer, adrenal tumors, or sudden cardiac death. Genetic testing reveals this to be a non-hereditary medullary thyroid cancer. His CT scans of his neck below reveal the suspicious right neck mass confirmed to be medullary thyroid cancer (arrow).His CT scan of his chest and neck do not reveal evidence of spread. His calcitonin is 3179 and his CEA is 18.6 before surgery.His surgery includes a total thyroidectomy, central compartment dissection and right anterolateral neck dissection. Right inferior parathyroid gland autotransplanted.
Pathology
Medullary thyroid cancer 1.4 cm
Central compartment dissection 4 of 22 lymph nodes with spread of medullary thyroid cancer
Right anterolateral neck dissection 6 of 36 lymph nodes with spread of medullary thyroid cancer
Three year follow up:
Calcitonin below any detectable levels
CEA 1.6 ng/ml
Ultrasound without any abnormalities
Patient is highly likely cured of his medullary thyroid cancer!!
Medullary Thyroid Cancer Surgery in Sites Other Than The Neck
Medullary thyroid cancer surgery is uncommonly proposed as a treatment approach when disease has spread to distant sites. Although surgery is not commonly proposed for distant spread of medullary thyroid cancer, consideration for surgery for distant disease is based upon the expert thyroid cancer team evaluation and considers the following issues:
- Where is the medullary thyroid cancer distant disease located?
- What are the risks and benefits of surgery?
- Are there other sites of distant spread?
- What medullary thyroid cancer treatments have already been used?
- What were the outcomes of other treatments for the medullary thyroid cancer?
- How fast is the medullary thyroid cancer growing?
- What are the patient's treatment desires?
- What are the other treatment options?
- What is the medullary thyroid cancer pathologic type (what do the cells look like under the microscope?
- What is the RET mutation associated with the medullary thyroid cancer?
Medullary Thyroid Cancer- Robotic Surgery Should Not Be Performed
Robotic surgery for the thyroid was developed largely in South Korea and brought to the United States several years ago as a "tool" in thyroid surgery. Its proposed benefits were to be the following:
- Absent or less noticeable neck incisions
- Improved visualization
- Less Surgeon Fatigue
Although we have been trained and performed robotic thyroid surgery, the following is the reality of robotic thyroid surgery:
- Incisions are tremendously longer but just not located on the front of the neck
- In medullary thyroid cancer, it is a one sided surgery approach to a both side of neck surgery!!!!
- The instruments used to perform the surgery are not as refined or delicate as the instruments used to perform the minimally invasive neck surgeries. (think of all the delicate structures that we have shown you here)
- Multiple surgeons are required
- The surgeon has no ability to "feel" in the neck. The fingers are the surgeon's third eye. Subtle changes in feel, hardness or extension of cancer can be totally unappreciated.
- It is not minimally invasive by any measure. It is maximally invasive but just at a distance from where the surgery is focusing.
- It is a much longer surgical procedure by any measure (the set up of the robot is longer than the average thyroid lobectomy).
- It is an inferior surgical approach to manage medullary thyroid cancer
- Unanticipated findings during surgery may not be able to be adequately addressed robotically.
Most importantly, the ability to perform a surgery is not an indication for a surgery!!! Robotic thyroid surgery is an inferior surgical approach in managing medullary thyroid cancer, any other type of thyroid cancer, or any thyroid lesion at risk of being a potential thyroid cancer.