Interesting Thyroid Cases
Interesting case of the week 6/17/22: Patient interviewed surgeons for years for her massive goiter before finding us on YouTube!
We're back for another edition of Royters Goiters with your very own Goiter Guru, Dr. Rashmi Roy!
Today's patient is a 49-year-old woman from South Carolina. She had been dealing with her massive goiter for a very long time and experiencing the typical symptoms we always talk about like difficulty breathing, swallowing and more.
She interviewed surgeons for years and never felt comfortable with any of them. After finding me on YouTube, she filled out a new patient form and decided to come see me for her surgery just a few weeks later.
Watch the full video to learn more details about her case, see footage of me removing her goiter in the operating room, review her pre-operative imaging and hear how she's doing now!
Interesting case of the week 6/10/22: Massive, one-sided thyroid goiter found incidentally with Dr. Rashmi Roy
We're back for another edition of Royters Goiters with your very own Goiter Guru, Dr. Rashmi Roy!
Today's patient is a 49-year-old man from South Carolina. His massive, one-sided thyroid goiter was found incidentally, meaning he was having no symptoms and the mass was discovered on a CT scan he had done for another reason.
Watch the full video to learn more details about his case, see footage of me removing her goiter in the operating room, review his pre-operative imaging and hear how he's doing now!
If you have a thyroid goiter, you need an expert evaluation at the Hospital for Endocrine Surgery. Click the "become a patient" button at the top of this website and fill out the form - we'll be in touch with you shortly to discuss the details of your case!
Interesting case of the week 6/3/2022 with Dr. Rashmi Roy: Thyroid goiter strangling patient - watch me remove it!
We're back for another edition of Royters Goiters with your very own Goiter Guru, Dr. Rashmi Roy!
Today's patient is a 42-year-old woman with a ten year history of her thyroid goiter. In recent years, she was having difficulty breathing to the point where she couldn't even walk to her mailbox without being out of breath. Her goiter was essentially strangling her and she needed surgery to relieve her of her symptoms.
Watch the full video to learn more details about her case, see footage of me removing her goiter in the operating room, review her pre-operative imaging and hear how she's doing now!
Interesting case of the week: A rare variant of papillary thyroid cancer and a rare congenital cyst with Dr. Nate Walsh
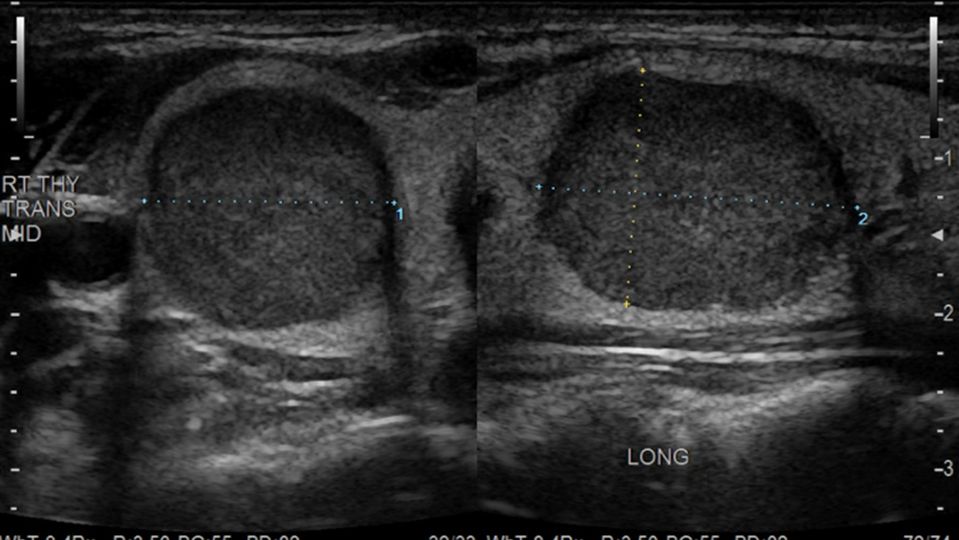
A 47- year- old gentleman was seen at our center for a suspicious nodule in the left half of his thyroid. Needle biopsy showed suspicious cells with a 15%-40% chance of cancer. He sought us out for expert evaluation.
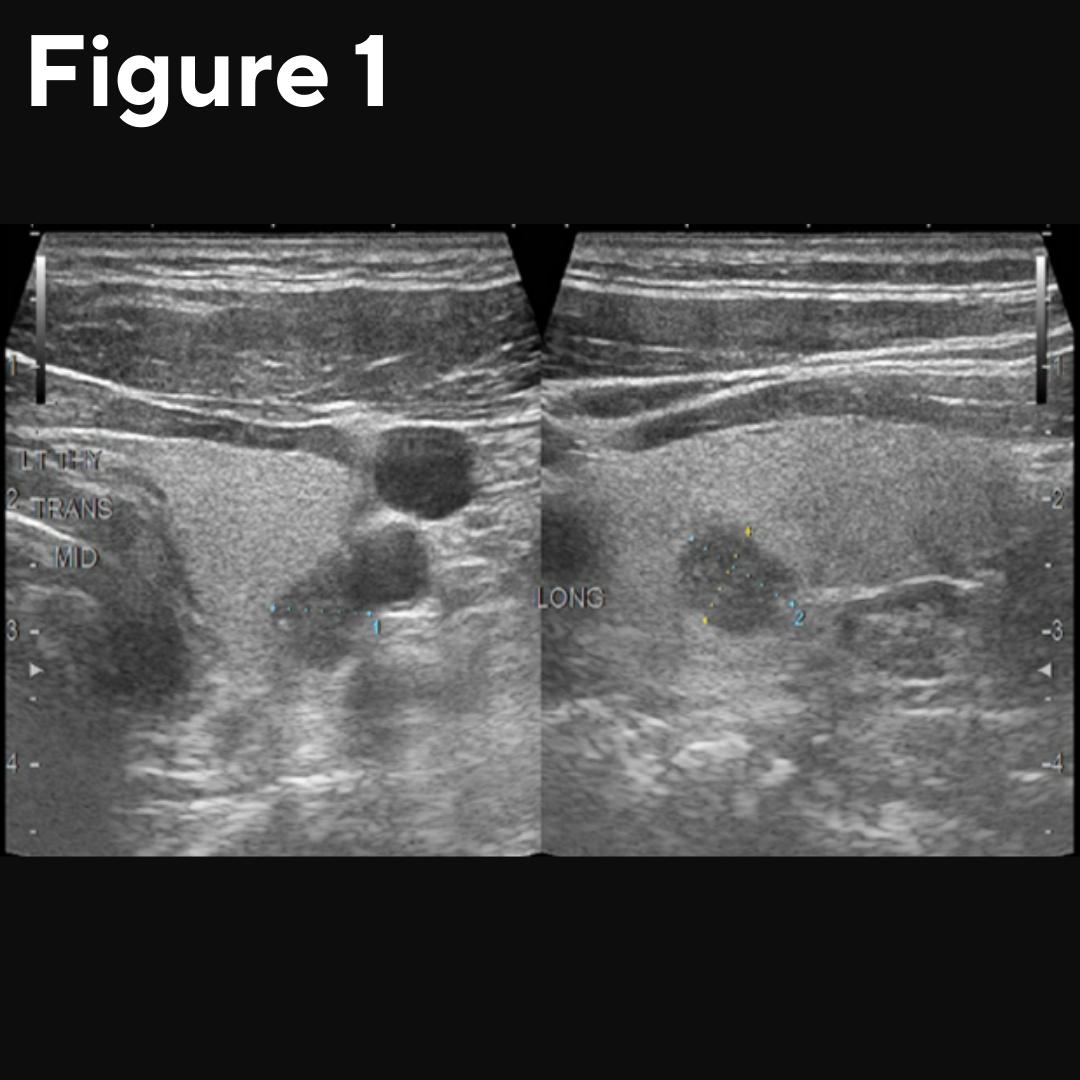
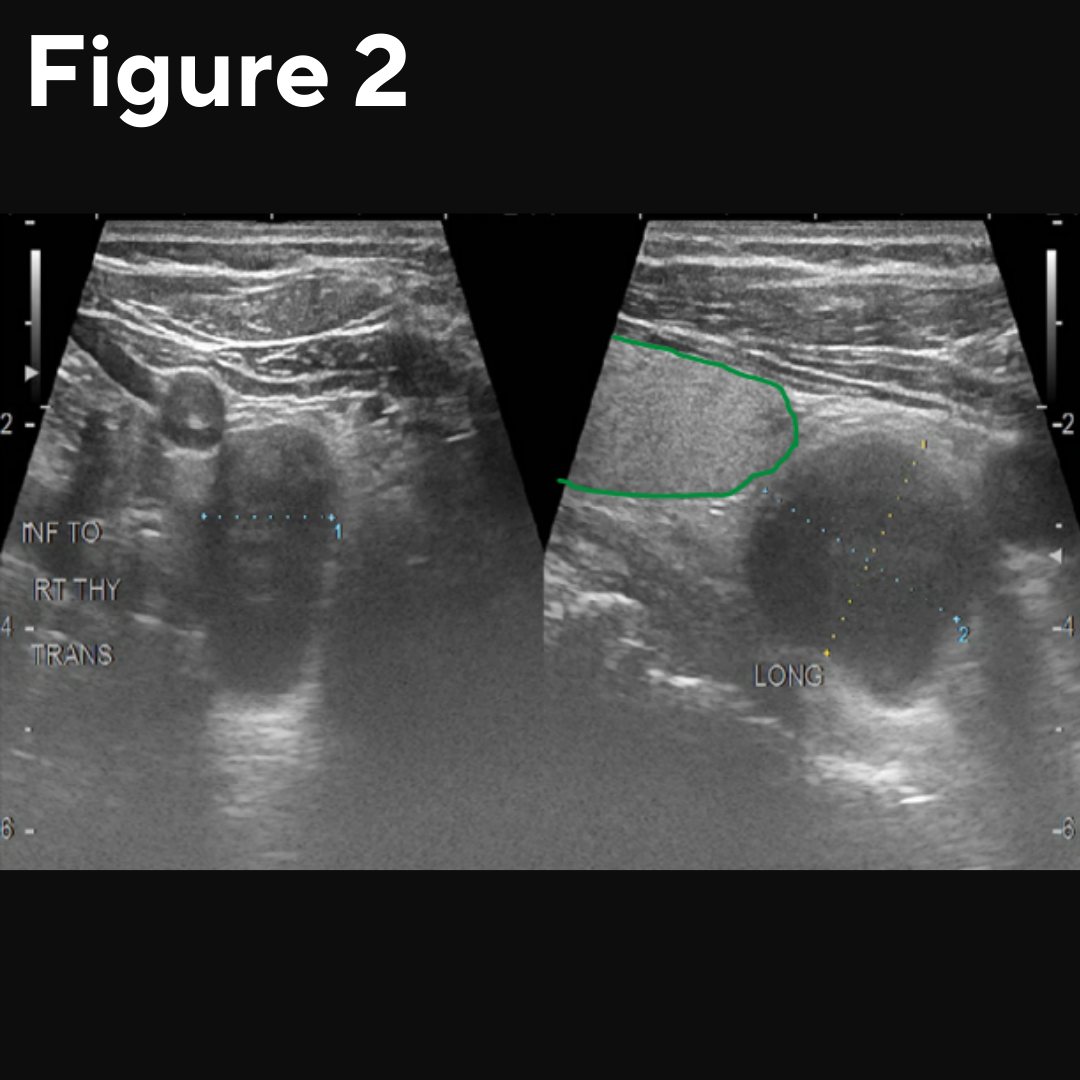
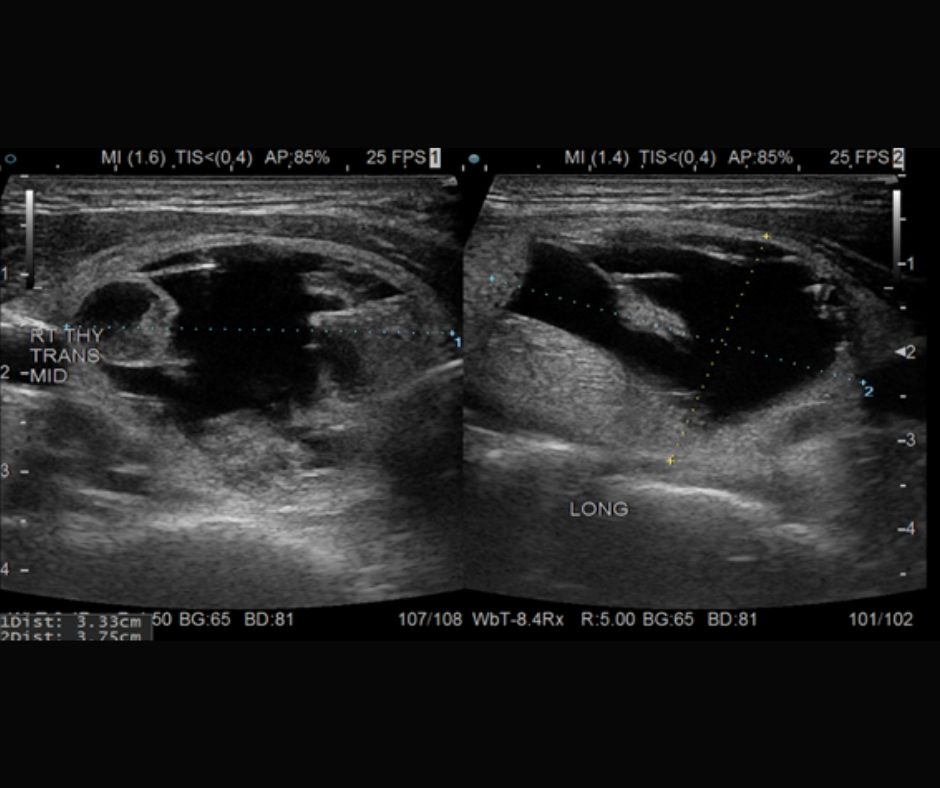
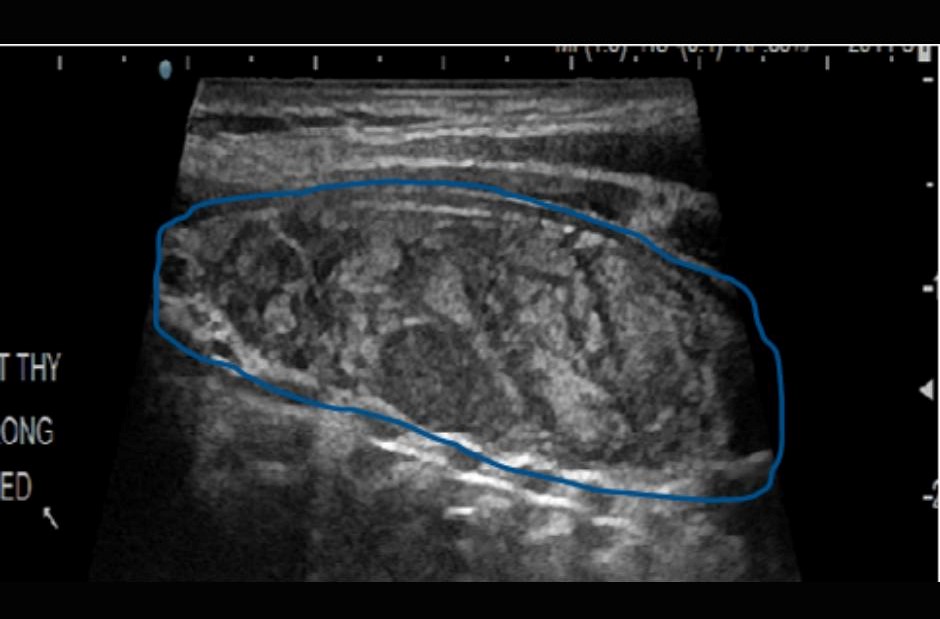
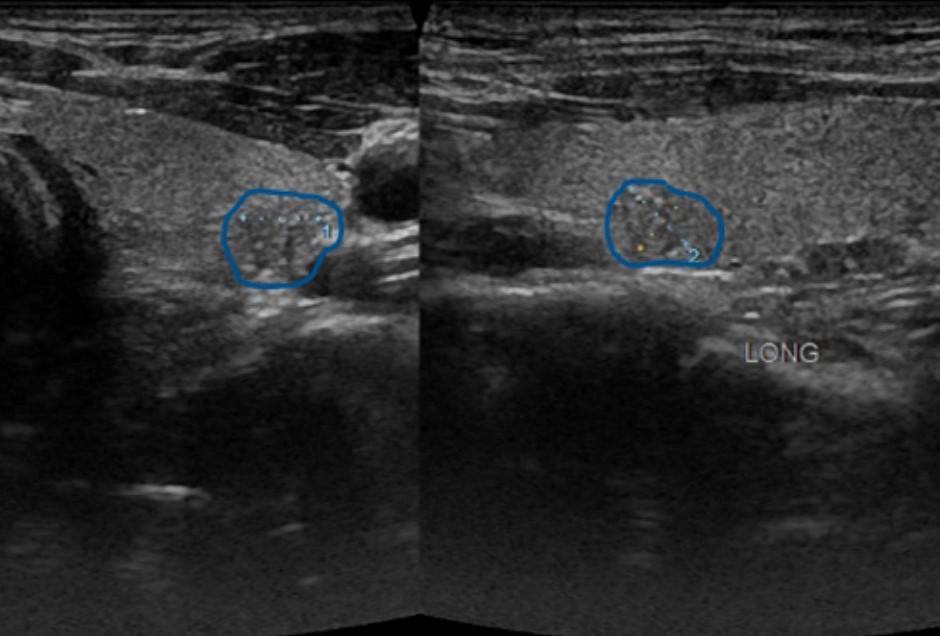
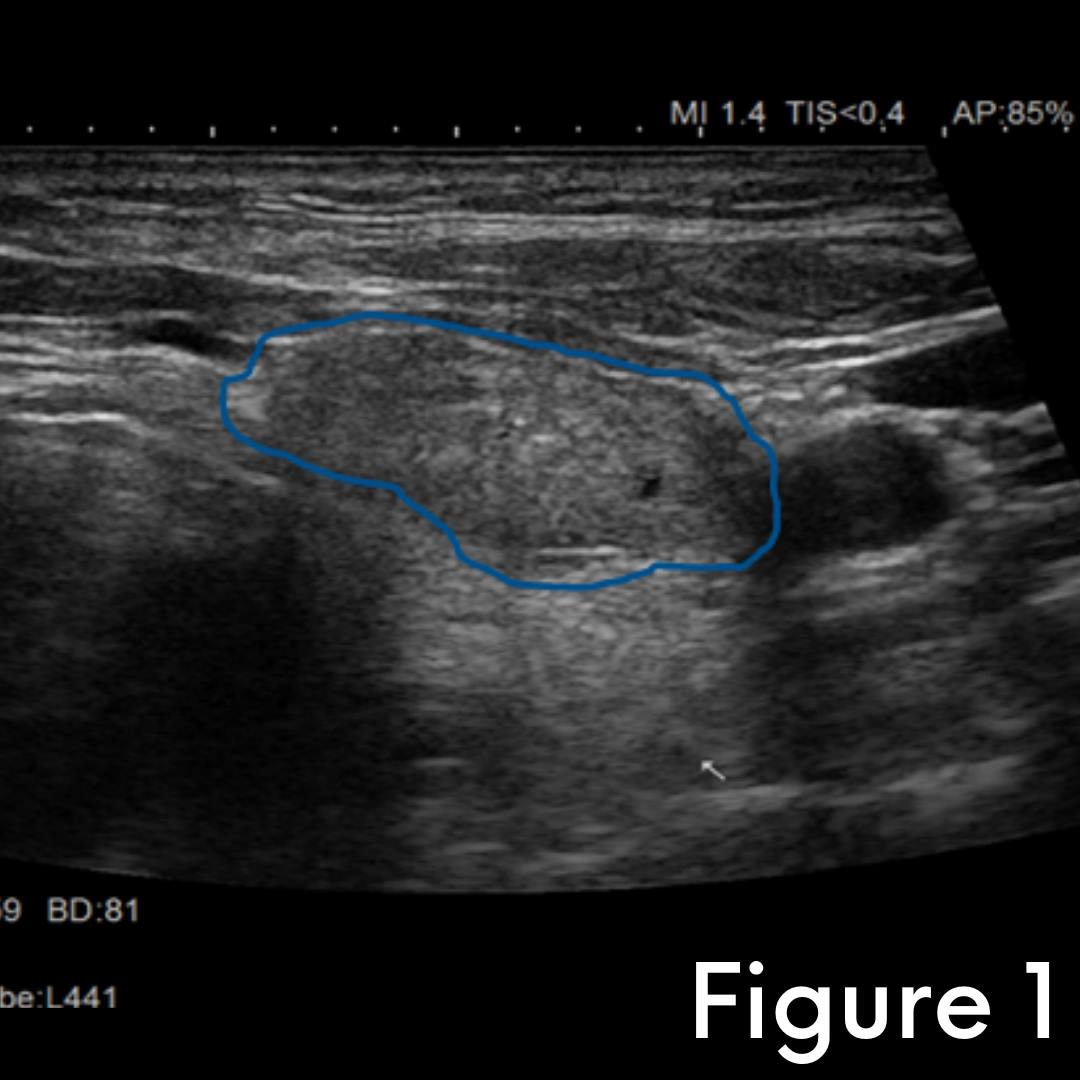
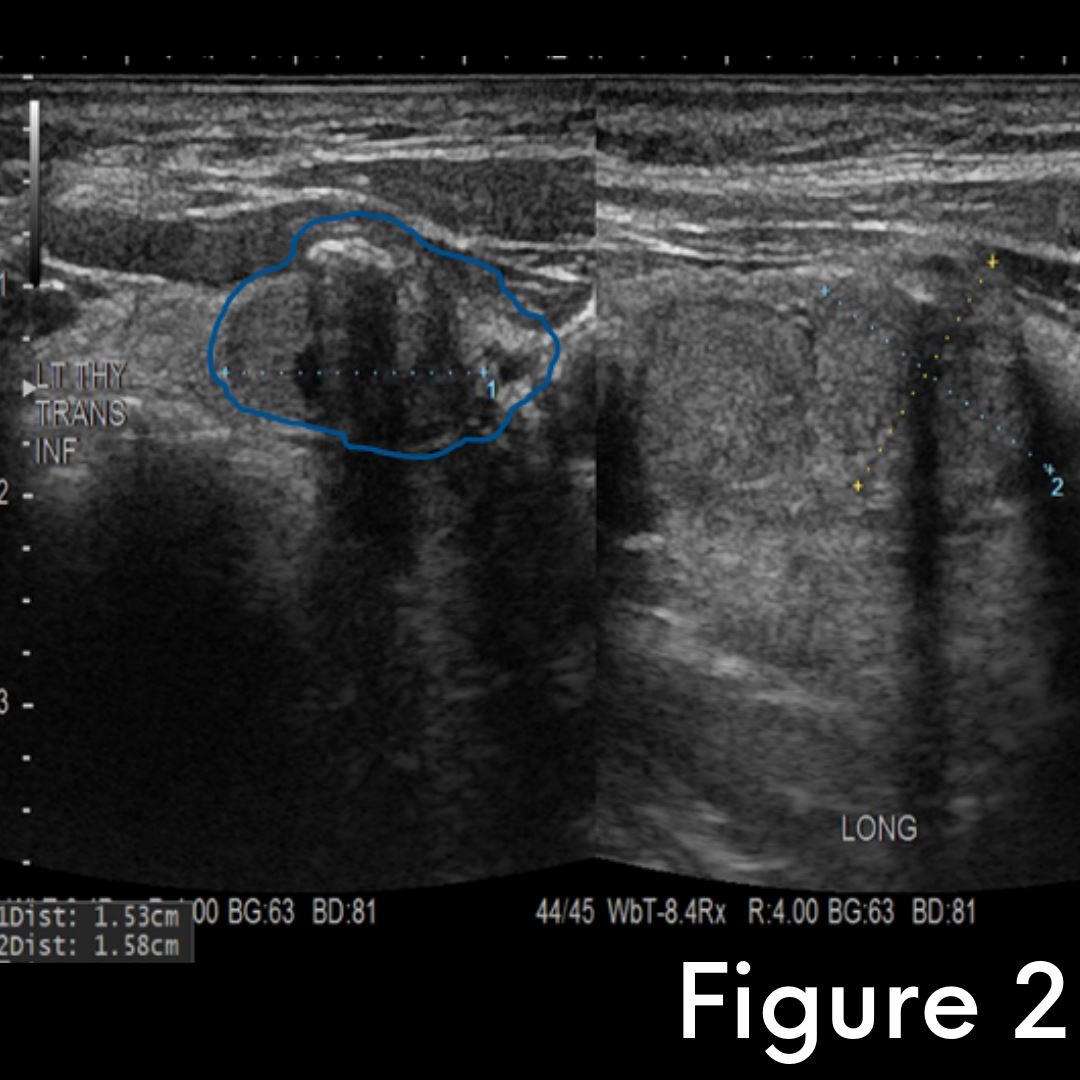
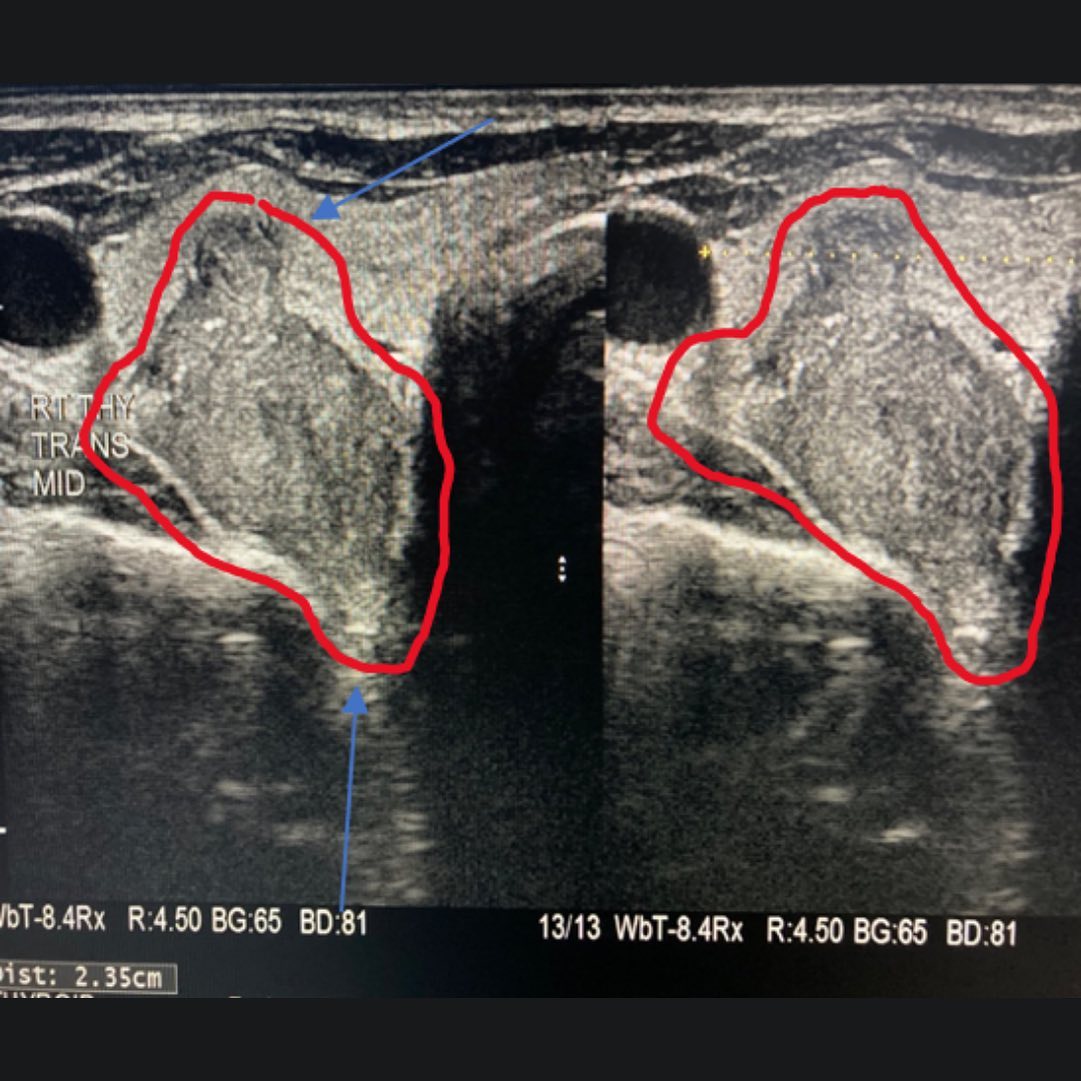
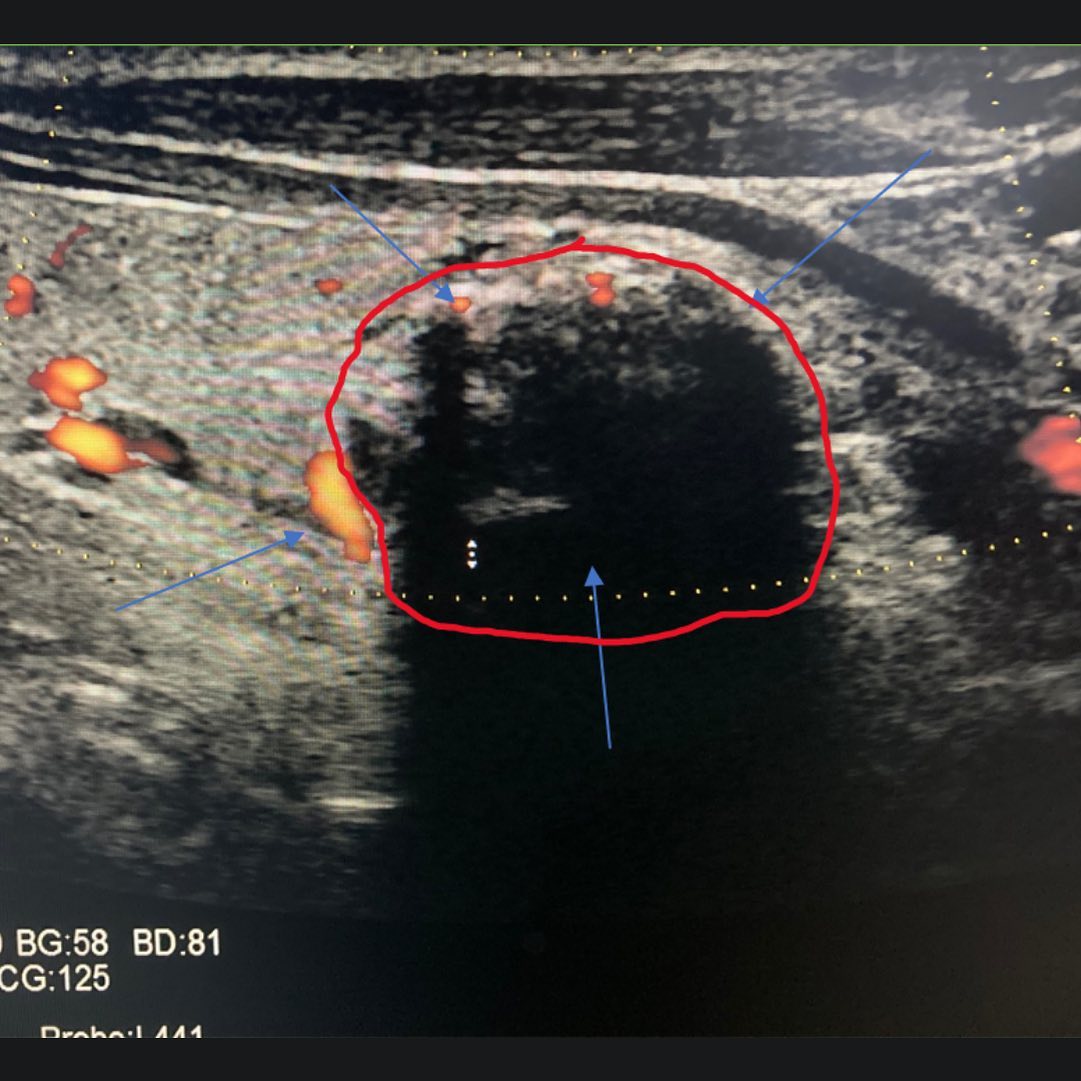
Upon our examination and work-up, we noted an irregular nodule in the left thyroid (Figure 1). This nodule was also suspicious due to its appearance and density/texture compared to surrounding tissue on ultrasound. There was no doubt this was a cancer until proven otherwise. Additionally, our world-class ultrasound team also located a mass in the right thyroid bed down below the thyroid towards the entrance to the chest cavity (Figures 2-3). This mass was not seen or located on imaging done prior to our evaluation. The density and appearance of the mass lead us to believe this was fluid-filled (cystic) and separate from the thyroid. Due to its size, appearance, and location, we performed a CT scan to better characterize the mass. CT scan confirmed a large, cystic mass in the right central compartment that was indeed separate from the thyroid. After discussion with the patient, we determined the best course of action was to also remove this mass and have the lesion analyzed by pathology in the operating room.
Figures 1 shows ultrasound images of the left thyroid nodule (measured with calipers)
Figures 2 shows ultrasound images of the right central neck mass (thyroid edge outlined in green)
Our patient underwent a successful surgery to remove the left side of the thyroid, the lymph nodes around the thyroid as well as the cystic mass.
Interestingly, the nerve to his voice box on the right side was very adherent to the right central neck mass we diagnosed during our work-up. This required very tedious microscopic dissection to ensure the tumor was completely removed while preserving the integrity and function of the nerve to the voice box on the right side. Real-time analysis of this mass during the operation revealed a rare, benign congenital cyst known as a bronchogenic cyst and benign lymph nodes. Real-time analysis of the lymph nodes behind the thyroid on the left revealed no cancer. As such, he was able to keep the right half of his thyroid. He experienced no change in voice, swallowing, or calcium regulation post-operatively.
Our patient did wonderfully during and after surgery and is recovering very nicely. His thyroid pathology showed that the suspicious left thyroid nodule was a rare variant of papillary thyroid cancer know has Tall Cell variant, which can behave more aggressively. The cancer was small (1cm), confined entirely to the thyroid, and had negative margins with no associated lymph node involvement. He is cured.
The large, rare, congenital cyst was certainly a surprising finding. These cysts arise from the respiratory tree during development as an embryo. While benign, the cysts can become symptomatic as they enlarge. Additionally, they can also lead to infection, particularly pneumonia. In some rare cases, these cysts can morph or degenerate into cancerous lesions over time. Given its size and the fact his cyst was stuck to a large section of the nerve to his voice box on the right side, he certainly would have developed symptoms or an issue with voice or swallowing.
Skill and experience are paramount when dealing with thyroid cancer, thyroid disease, and thyroid surgery. This is especially true in the management of rare tumors or a cancer that are stuck on, or growing into, the nerves to the voice box. These critical nerves of the voice box that control sensation and movement of the vocal cords must be identified and preserved in every thyroid operation. Had his surgery been performed elsewhere by an inexperienced surgeon, our patient almost certainly would have had permanent damage to the nerve to the voice box on the right due to its close involvement with this rare tumor.
Interesting case of the week 5/6/2022 with Dr. Rashmi Roy: Patient underwent total thyroidectomy 20 years ago, but scans now show a substernal goiter
Today's case is a bit of a mystery!
This patient was told she had her entire thyroid removed 20 years ago. She had a scan done for another reason which showed a large thyroid goiter growing down into her chest, so she decided to come see me.
Watch the full video to hear more about her case, see footage of me in the operating room and find out if it was indeed her thyroid!
Interesting case of the week 4/29/2022 with Dr. Rashmi Roy: Huge Graves' goiter wrapping around windpipe
Today I want to tell you about a young gentleman with significant Graves' disease and a huge thyroid -- this is called a Graves' goiter.
Graves' can be treated either medically or surgically. Surgery is the only curative option, and it was necessary for this patient because his goiter was wrapping around his windpipe and causing voice changes, difficulty breathing and swallowing, and snoring among other symptoms.
Watch the full video to hear more about his case, review his imaging to see how the goiter was wrapping around his windpipe, see footage of me removing his goiter in the OR and more.
Interesting case of the week 4/15/2022 with Dr. Rashmi Roy
We're back for another edition of Royters Goiters with our very own Goiter Guru, Dr. Rashmi Roy!
In this week's interesting case, we have a mother from Texas with three young children at home. She was struggling with typical symptoms related to a massive thyroid goiter. She visited three different surgeons who all told her they would need to crack her chest and perform a sternotomy in order to remove the goiter. She was understandably apprehensive about having her chest cracked and continued searching for other options.
She found me on YouTube and ended up cancelling her scheduled surgery elsewhere to come to Tampa and see us.
Watch the full video to hear more details about her case, see footage of me in the operating room removing the goiter, and more: https://youtu.be/15LrYU5u7Vc
We are so happy this patient is no longer struggling with her thyroid goiter and did not have to undergo a sternotomy!
Interesting case of the week 4/8/2022: A Rare Neuroendocrine Tumor Masquerading as a Suspicious Thyroid Nodule with Dr. Nate Walsh
A 66-year-old lady was seen at our center for multiple thyroid nodules in both sides of her gland. The most concerning nodule was in the right half (lobe) of her thyroid, and this mass had an indeterminate result on needle biopsy. Further molecular/genetic testing of the cells from the biopsy revealed a 50% chance of cancer. She came in from out of state to seek consultation and surgical treatment at our center of excellence.
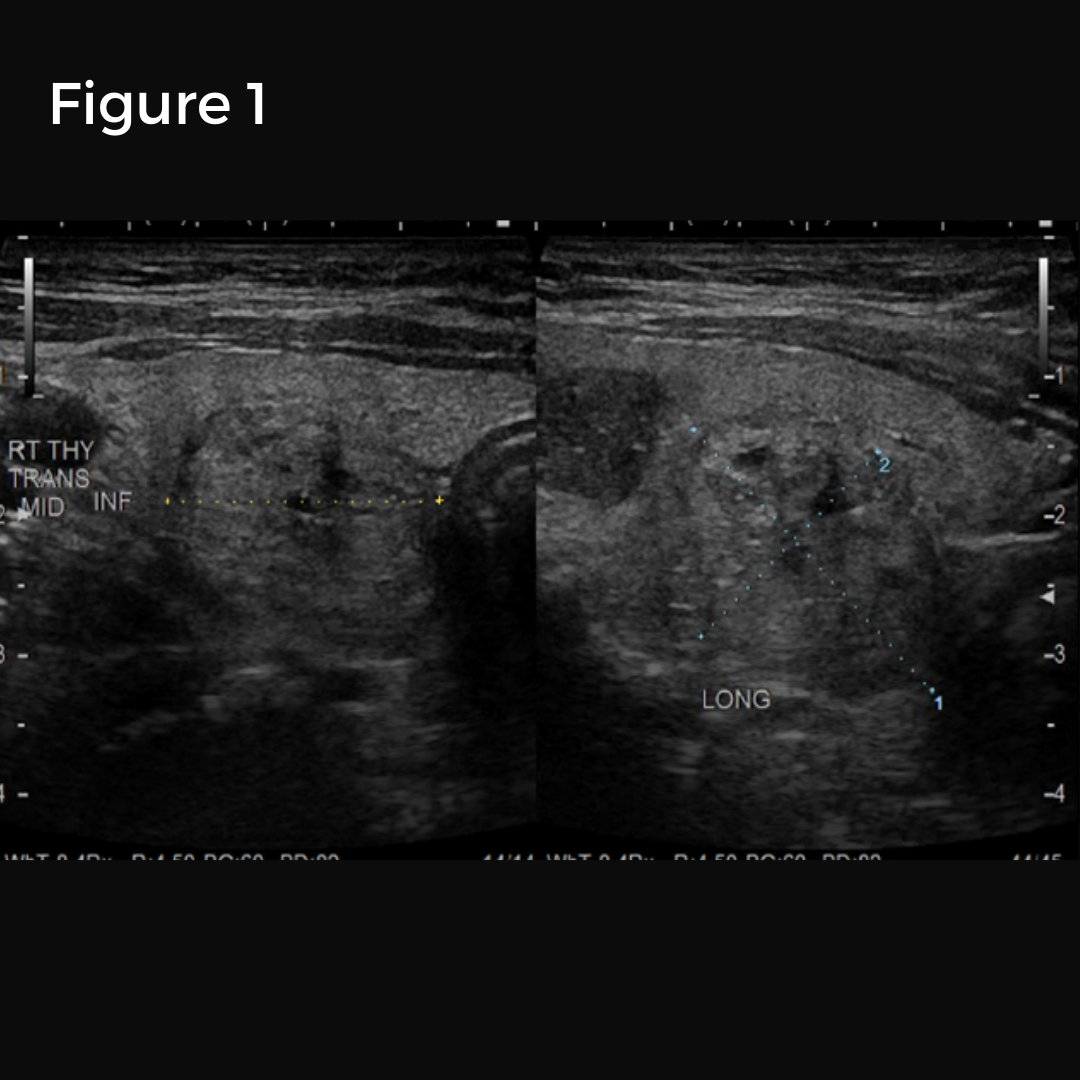
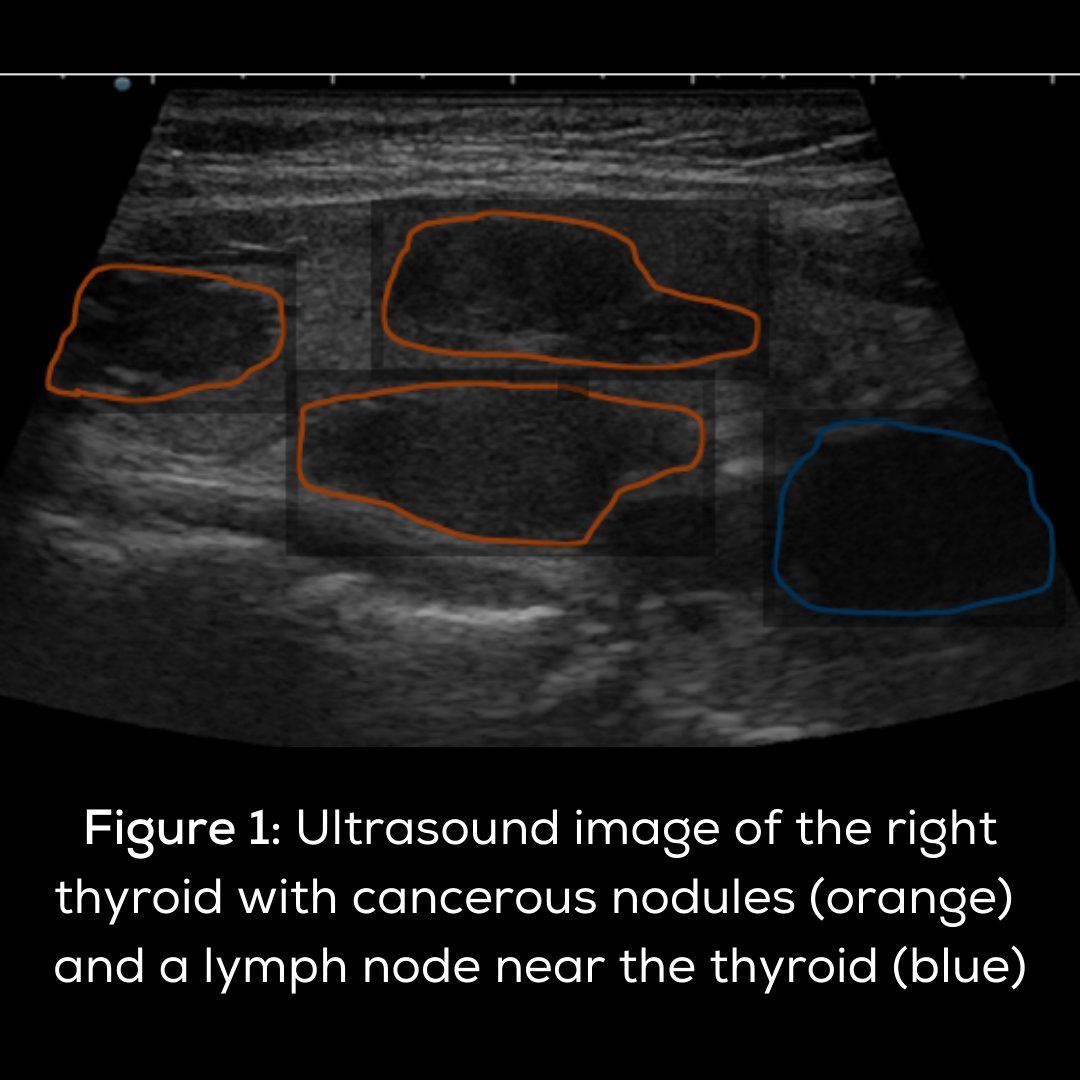
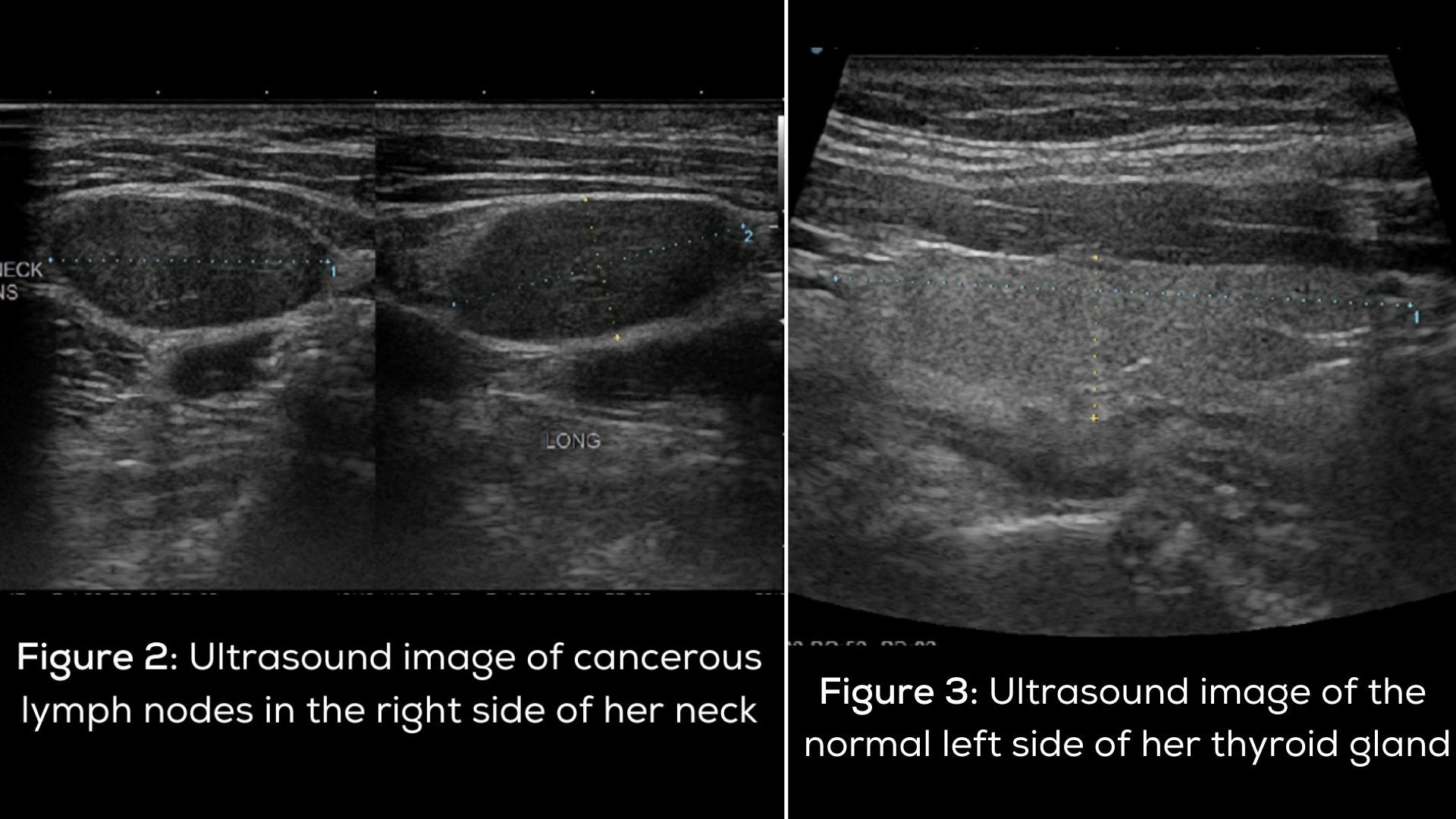
Upon our examination and work-up, we noted multiple sizable nodules in both sides of her thyroid. On our ultrasound, the nodule with the most concerning features was the one in the right lobe. We did not see any suspicious lymph nodes in either side of the neck. Due to the size and appearance of her nodules and the aforementioned molecular/genetic test results of the one on the right side, she elected to proceed with removal of her entire thyroid gland (total thyroidectomy) along with the lymph nodes around/behind the thyroid gland. This would allow for a definitive diagnosis while ensuring she was cured of these nodules, even if a cancer was present.
Figures 1 shows ultrasound images of the right thyroid nodules.
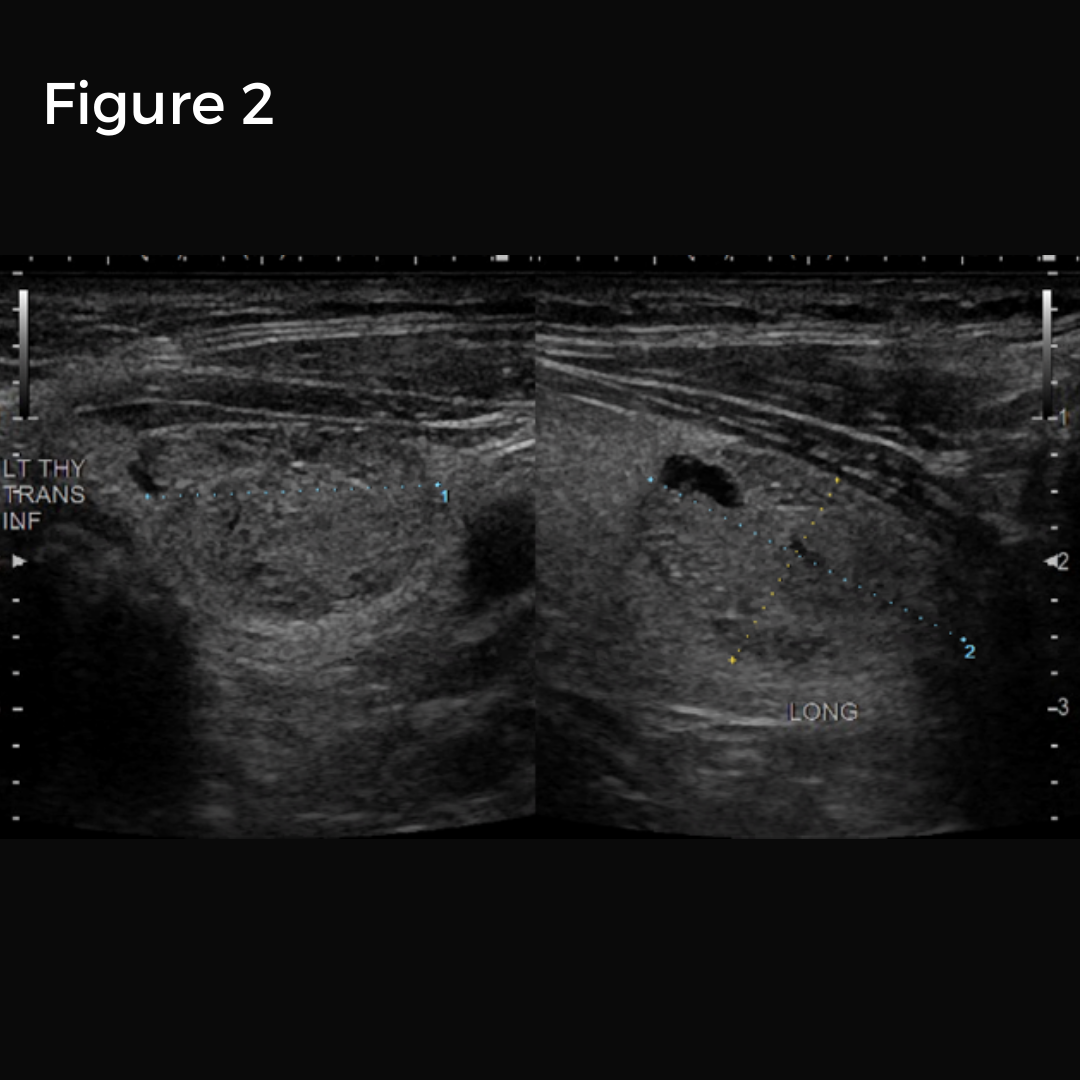
Figure 3 shows ultrasound image of the large left thyroid mass.
Our patient underwent a successful surgery to remove her entire thyroid gland and the lymph nodes behind and around the thyroid on both sides. Surprisingly, the nerve to her voice box on the right side was coursing through, and very adherent to, the concerning mass that had been biopsied. This required very tedious microscopic dissection to ensure the tumor was completely removed while preserving the integrity and function of the nerve to the voice box on the right side. She experienced no change in voice, swallowing, or calcium regulation post-operatively. Her physical appearance will remain unaltered except for the small, well- designed scar located in the lower portion of her neck.
Our patient did wonderfully during and after surgery and is recovering very nicely. Her pathology interestingly showed that the suspicious mass in her right thyroid that was very stuck on the nerve to her voice box was actually an extremely rare neuroendocrine tumor known as a paraganglioma. These tumors can be benign or cancerous, and they involve nerves in the body that are outside of the brain and spinal cord. While hers was benign and not symptomatic, some of these rare tumors can cause symptoms if cancerous or by producing and secreting various hormones. Additionally, these tumors are associated with genetic or inherited syndromes. Of note, all of her other thyroid nodules and the lymph nodes were negative for cancer.
Skill and experience are paramount when dealing with thyroid cancer, thyroid disease, and thyroid surgery. This is especially true in the management of tumors or cancer that are stuck on, or growing into, the nerves to the voice box. These critical nerves of the voice box that control sensation and movement of the vocal cords must be identified and preserved in every thyroid operation. Had her surgery been performed elsewhere by an inexperienced surgeon, our patient almost certainly would have had permanent damage to the nerve to the voice box on the right due to its close involvement with this rare tumor. Furthermore, the parathyroid glands that control calcium in the body must also be identified and spared during all thyroid operations. All of this is to say that only expert, high-volume surgeons should perform thyroid surgery, particularly when tumors or cancer involve the nerves to the voice box.
Expert and experienced evaluation, treatment, and follow-up for thyroid disease and thyroid cancer is of paramount importance.
Interesting case of the week 4/1/2022 with Dr. Rashmi Roy
We're back for another edition of Royters Goiters with our very own Goiter Guru, Dr. Rashmi Roy!
Today we have a 56-year-old woman with two things going on - she had a very large thyroid goiter that was producing a lot of thyroid hormone. This is called a toxic multinodular goiter. The goiter was growing up and into her jaw as well as down and into her chest. Her thyroid hormone being so out of control was causing her to shake, lose weight and have difficulty sleeping.
Watch the full video to see footage of me in the operating room removing this massive thyroid goiter, review her imaging and hear how she's doing now.
Interesting case of the week 3/18/2022: Metastatic Papillary Thyroid Cancer: Why Expert Ultrasound is Crucial
This week, a 21-year-old woman was seen at our center for papillary thyroid cancer. She had a 1.3 cm papillary thyroid cancer on the left side diagnosed with an ultrasound and needle biopsy at an outside facility. The plan was to remove the left half of her thyroid gland to treat this cancer.
After doing their own research online, she and her family desired a second opinion at our center. They traveled from out of state to seek care at our facility.
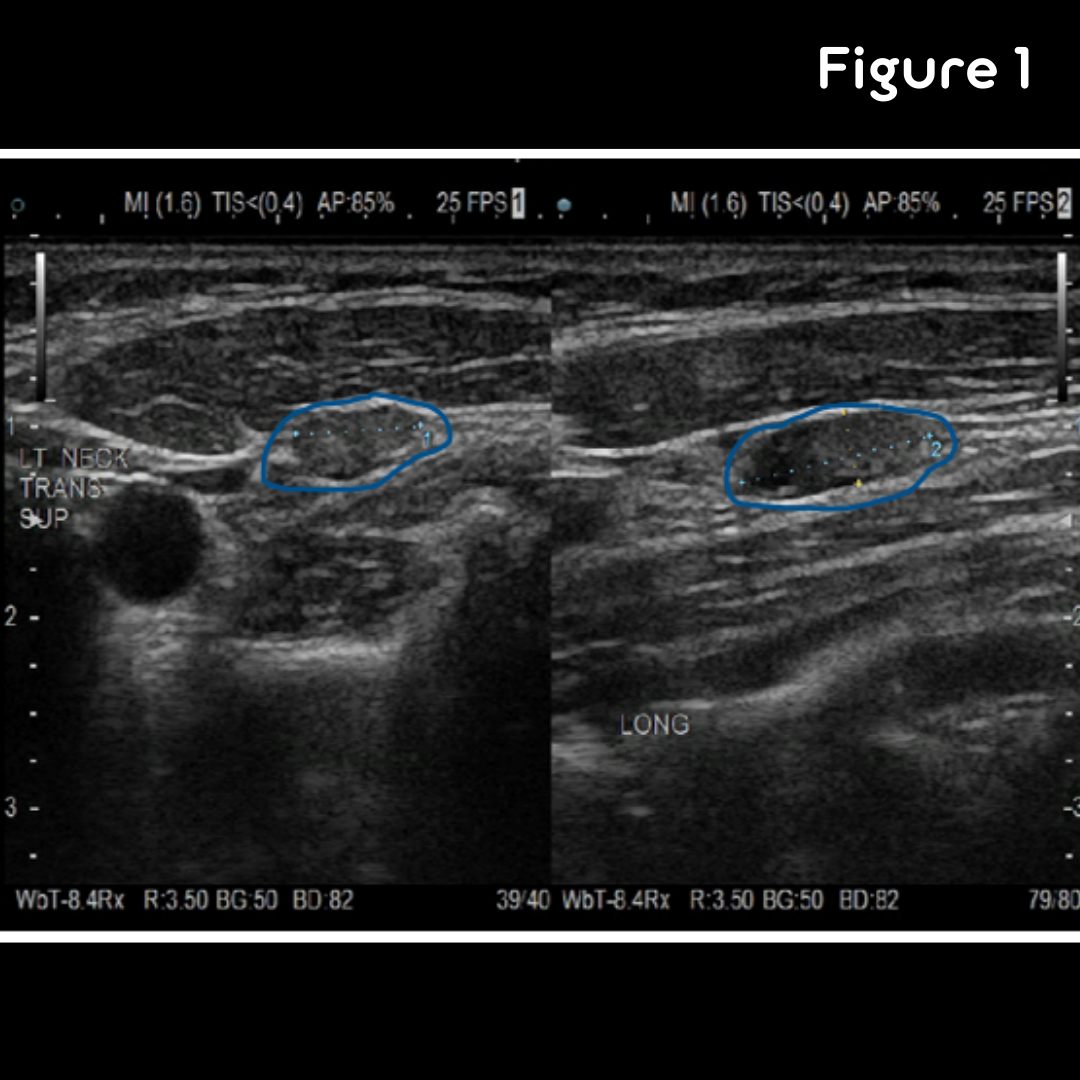
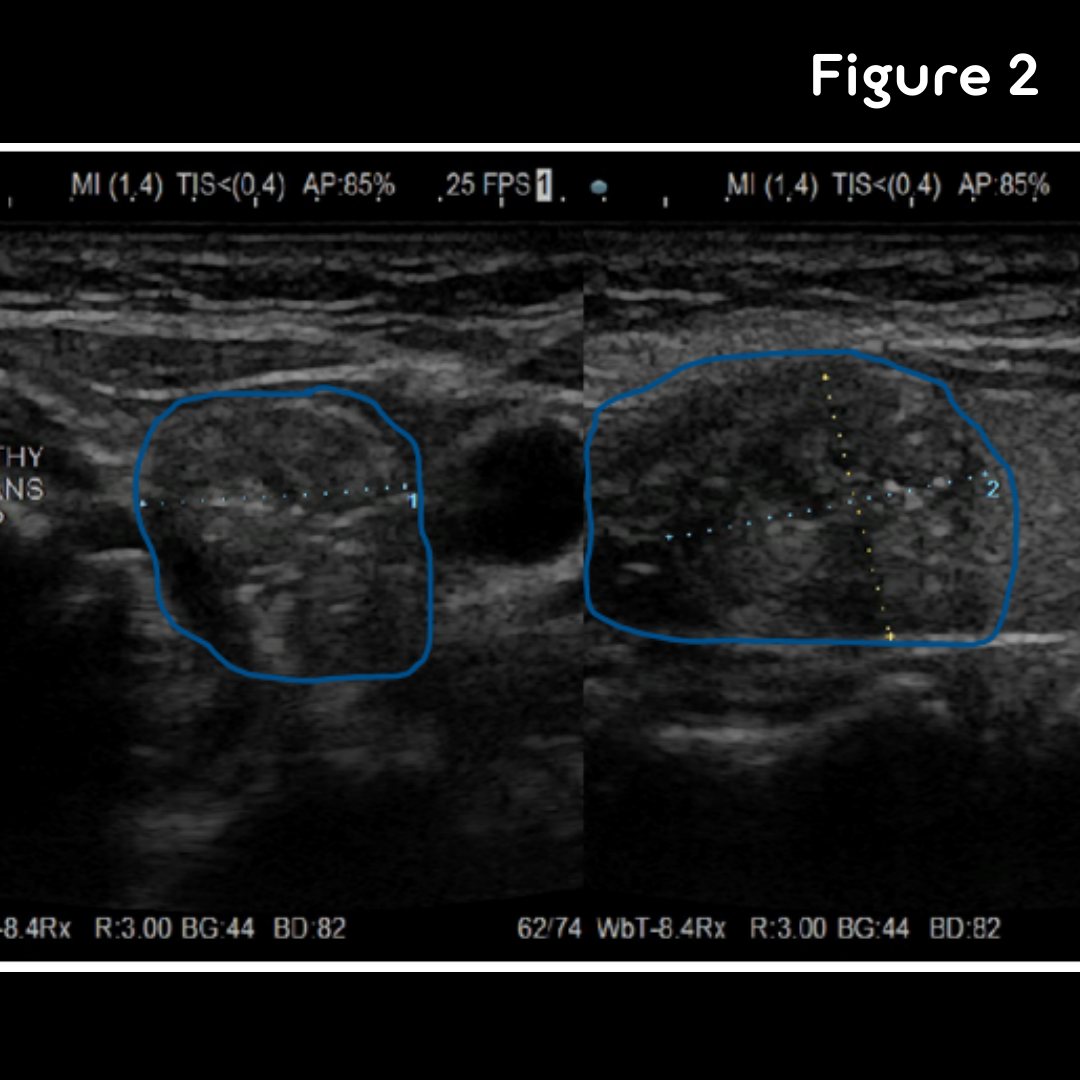
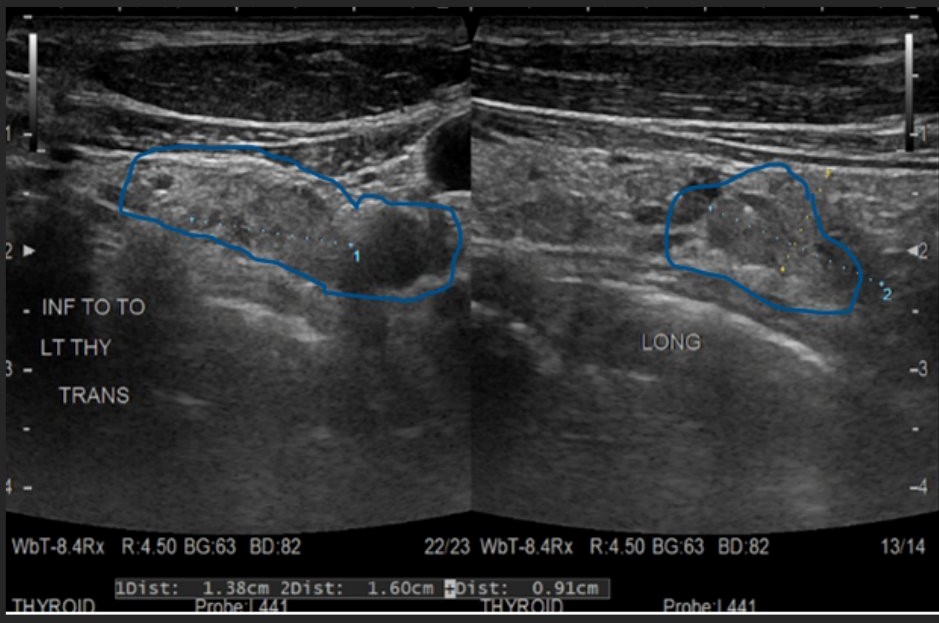
At our evaluation, we performed a thorough ultrasound to evaluate her thyroid and the lymph node areas in the neck associated with thyroid cancer. She had concern for not only a left-sided thyroid cancer, but other smaller foci of cancer throughout her thyroid. Additionally, this young lady had multiple suspicious lymph nodes around/behind her thyroid on the left as well as in the left side of her neck.
Figures 1: Ultrasound images of the left neck. Blue highlights enlarged, suspicious lymph nodes
Figure 2: Ultrasound images demonstrating her thyroid cancer outlined in blue. Irregular borders and shadowing from tiny calcifications are noted.
A needle biopsy of a suspicious lymph node in the left side of her neck confirmed metastatic papillary thyroid cancer. A CT scan of her neck was done as well prior to surgery. She would need a large operation to cure her cancer. This young lady underwent a total thyroidectomy (complete removal of the thyroid gland) combined with removal of the lymph nodes around and behind the thyroid on both sides as well as all the lymph nodes in the side compartment of her left neck. Final pathology confirmed a left papillary thyroid cancer with multiple smaller, satellite cancers in the left and right side of the thyroid (multifocal). The cancer had also spread to multiple lymph nodes around/behind the thyroid as well as to lymph nodes in the left side of her neck. She experienced no change in voice or swallowing, calcium control (parathyroid glands were healthy). Her physical appearance will remain unaltered except for a scar located in the lower portion of her neck. She did wonderfully during and after surgery and is recovering very nicely.
Expert and experienced evaluation of thyroid cancer is of paramount importance. Critical to the evaluation of patients with thyroid disease is a detailed, complete ultrasound to examine the thyroid along with the lymph nodes in the neck that can be affected by thyroid cancer and thyroid disease. Our patient was misdiagnosed prior to her work-up at our center. This young lady had metastatic thyroid cancer that affected the lymph nodes not only around/behind the thyroid on the left (that are typically not removed by most surgeons), but also the lymph nodes in the left side of the neck. Prior to evaluation at our center, she was told she only needed half of her thyroid removed to cure her cancer. Only our expert, highly-experienced ultrasound team was able to diagnose the other areas of cancer in the thyroid along with the lymph node spread of this cancer. Had she not sought evaluation at our center of excellence, she would have had the wrong operation that left significant amount of cancer behind leading to further surgery.
This case also underscores the importance of healthcare providers understanding thyroid cancer. Younger patients with papillary thyroid cancer often have lymph node spread at the time of diagnosis. A thorough, expert ultrasound to evaluate all the lymph node areas in the neck is of critical importance. This combined with a CT scan of the neck to provide an anatomical road map for the operation are paramount. If a clinician does not look or does not know what he or she is looking for, thyroid cancer that has spread to lymph nodes will be missed.
Interesting case of the week 3/11/2022 with Dr. Rashmi Roy
We're back for a very special edition of Royters Goiters with our very own Goiter Guru, Dr. Rashmi Roy.
This week, Dr. Roy operates on a YouTube follower who wanted to share her story in hopes of reaching others in similar situations.
Meet Tammy, a woman who had been struggling with her thyroid goiter for many years and suffering from classic symptoms like difficulty breathing and swallowing. Over the years, the goiter grew larger and larger until it was impossible to ignore.
Tammy lives in the Midwest and wasn't able to find a surgeon she was comfortable with... until she came across Dr. Roy's YouTube channel!
Watch the full video to hear directly from Tammy, see footage of her in the operating room, review her imaging, and more.
To become Dr. Roy's patient, fill out the form at this link.
Dr. Rashmi Roy, Senior Surgeon at the Clayman Thyroid Center & Hospital for Endocrine Surgery, is unquestionably one of the most experienced thyroid surgeons in the US. Dr. Roy operates on a significant number of patients with thyroid goiters, many of whom other surgeons refuse because of their complexities.
Interesting case of the week 3/4/2022 with Dr. Rashmi Roy
We're back for another edition of Royters Goiters with our very own Goiter Guru, Dr. Rashmi Roy!
Today we have a young woman who knew about her goiter for years, but was afraid to have surgery. Eventually, her goiter was bulging out to a point she couldn't ignore and her symptoms were rapidly worsening.
Our patient lived in Pennsylvania and after tireless research, she decided she did not feel comfortable with any of the surgeons near her. She found us online and after reading through our website and watching Dr. Roy's videos on YouTube, she contacted us for an evaluation.
Watch the full video to hear more about her case, see footage of Dr. Roy in the operating room, review her imaging and more.
To become Dr. Roy's patient, fill out the form at this link.
Dr. Rashmi Roy, Senior Surgeon at the Clayman Thyroid Center & Hospital for Endocrine Surgery, is unquestionably one of the most experienced thyroid surgeons in the US. Dr. Roy operates on a significant number of patients with thyroid goiters, many of whom other surgeons refuse because of their complexities.
Interesting case of the week 2/25/2022 with Dr. Rashmi Roy
We're back for another edition of Royters Goiters with our very own goiter guru, Dr. Rashmi Roy!
We've covered thyroid goiters that grow down into the chest (substernal goiters), but today we have a goiter that was growing up and into the jaw.
Watch the full video to see her pre-op photos, footage of Dr. Roy in the operating room, review her imaging and more!
Thyroid goiters come in all shapes and sizes, and remember, they are NOT always benign. All goiters require expert evaluation. If you have a thyroid goiter, schedule an evaluation with Dr. Roy here.
Interesting case of the week 2/18/2022: Metastatic Medullary Thyroid Cancer with Dr. Nate Walsh
This week, a 38- year- old woman was seen at our center for known medullary thyroid cancer with spread to the lymph nodes within her neck. Over the past 10-12 months, she had seen multiple doctors for a lump in her right neck. Multiple clinical visits included treatment for infectious and inflammatory causes of enlarged lymph nodes. When these attempts failed to improve the lumps in her neck, she ultimately was referred to a local cancer center.
Numerous blood and imaging tests were performed, including a CT scan and a PET/CT scan. She also had a needle biopsy of a lymph node in the right side of her neck that confirmed that the medullary thyroid cancer spread to lymph nodes in her right neck (metastatic). There was no evidence of spread of the cancer outside of her neck (distant metastases), thus making this a locally-advanced cancer. Finally, genetic testing revealed that she did not have an inherited type of medullary thyroid cancer.
Her case was presented and discussed at the outside cancer center’s tumor board with numerous doctors and clinicians participating. The “cancer surgeon” ultimately told the patient that this cancer was not able to be treated with surgery because the thyroid tumor and involved lymph nodes were too close to the windpipe, esophagus, and nerves near her spine. Thus, they recommended chemotherapy and radiation. She frantically sought a second opinion and reached out to our expert thyroid center.
Upon our examination and work-up, we noted multiple areas of cancer in the right side of her thyroid along with several enlarged cancerous lymph nodes around and behind the right half of her thyroid and in the right side of her neck. The left side of her thyroid and lymph nodes in the left side of her neck were completely normal. We reviewed imaging studies, including her CT scan from the outside facility and determined her medullary thyroid cancer could be completely removed safely without taking out or damaging her windpipe, esophagus, or nerves near her spine.
Our patient underwent a successful surgery to remove her entire thyroid gland and the lymph nodes behind and around the thyroid on both sides along with the lymph nodes in the right side of her neck. She experienced no change in voice, swallowing, or calcium regulation. Our patient did wonderfully during and after surgery and is recovering very nicely. Her pathology confirmed medullary thyroid cancer in multiple locations in her right thyroid lobe. 23 of the 66 lymph nodes in her neck had metastatic medullary thyroid cancer. She does not require chemotherapy or radiation therapy to control her medullary thyroid cancer that had once existed in her neck.
Skill and experience are paramount when dealing with thyroid cancer, thyroid disease, and thyroid surgery. This is especially true in the management of medullary thyroid cancer. The critical nerves of the voice box that control sensation and movement of the vocal cords must be identified and preserved in every thyroid operation. In addition, the parathyroid glands that control calcium in the body must also be identified and spared. Finally, the windpipe, esophagus, and important nerves and blood vessels in the side of the neck must be spared during a large operation like the one our patient underwent successfully.
Should our patient have started treatment with chemotherapy and radiation, as was recommended at the outside cancer center, her outcome, survival, and morbidity would almost certainly would have been worse.
Interesting case of the week 2/11/2022: Are thyroid goiters always benign?
We're back for another edition of Royters Goiters with your Goiter Guru, Dr. Rashmi Roy.
Today we have a 41-year-old woman who noticed a mass in her neck about six months prior to seeing me. Her symptoms developed to the point where she could barely breath.
I've told you about difficulty breathing before.... so, what makes this case interesting?
Final pathology revealed she had a 2 cm cancer within her goiter. When people hear "goiter", they often assume it's benign. The fact is, we find thyroid cancer in goiters 50% of the time. This is why it's so important to get your multinodular goiter evaluated by an expert.
Watch the full video to hear more about this patient's case, see her in the operating room, review her imaging and learn more about her outcome.
Dr. Rashmi Roy, Senior Surgeon at the Clayman Thyroid Center & Hospital for Endocrine Surgery, is unquestionably one of the most experienced thyroid surgeons in the US. Dr. Roy operates on a significant number of patients with thyroid goiters, many of whom other surgeons refuse because of their complexities.
Interesting case of the week 2/4/2022: Medical Tourism with Dr. Nate Walsh
This week, a 38-year-old woman from over 1000 miles away was seen for a second opinion on a right-sided papillary thyroid cancer. A lump in her neck had been noted on physical exam, and ultrasound along with a needle biopsy revealed papillary thyroid cancer. Subsequently, she was referred to a local surgeon.
She was told her whole thyroid needed to be removed for a cure. Consequently, she would then be on medication for the rest of her life. Additionally, the surgery to remove her entire thyroid would be riskier since both sides of her neck would be operated on, exposing all the nerves to the voice box and all four parathyroid glands to surgery and the potential for damage. Thankfully, she sought an expert evaluation at the Clayman Thyroid Center at the Hospital for Endocrine Surgery.
At our clinical visit, the ultrasound demonstrated a 2 cm mass in her right thyroid along with a few concerning lymph nodes near the cancer. The lymph nodes in each side of her neck were normal, indicating this cancer could be very likely be treated by removing half of the thyroid and the lymph nodes around the right thyroid. Her ultrasound images can be seen here.
Our young lady underwent a right #thyroidectomy along with the lymph nodes around the right half of the thyroid. Thankfully, rapid intra-operative pathology revealed no cancer in the lymph nodes. Thus, she was able to keep the healthy left half of her thyroid. She experienced no change in voice, swallowing, or calcium control. Our patient did wonderfully during and after surgery and is recovering nicely.
People traveling for the best medical care is becoming increasingly popular. While some patients seek medical attention locally or abroad to reduce cost, this comes with substantial risk. Nothing is more important than your health.
Our patient would have had too much surgery had she not come to our specialty center. Expert and experienced evaluation, surgery, and follow-up for thyroid cancer is of critical importance. Distance should not be the deciding factor in your thyroid care.
Interesting case of the week 1/28/2022: The importance of checking your own neck with Dr. Rashmi Roy
We're back for another edition of Royters Goiters, as we wrap up #GoiterAwarenessWeek with our very own Goiter Guru!
This week, Dr. Roy is taking you into the operating room as she removes a massive cancerous growth.
So, what makes this case interesting? This patient's mass had been growing for 10+ years, but he had no idea. This case underscores the importance of performing self checks on a regular basis. Not sure how to perform a self check? Check out Dr. Roy's instructional video here.
Dr. Rashmi Roy, Senior Surgeon at the Clayman Thyroid Center & Hospital for Endocrine Surgery, is unquestionably one of the most experienced thyroid surgeons in the US. Dr. Roy operates on a significant number of patients with thyroid goiters, many of whom other surgeons refuse because of their complexities.
Interesting case of the week 1/21/2022: A multinodular goiter growing significantly into the chest with Dr. Rashmi Roy
We're back with the goiter guru!
This patient's multinodular goiter grew substantially into his chest. He was told by other surgeons that his chest would need to be cracked in order to remove it. We were able to successfully remove this goiter through a standard neck incision. He suffered zero complications and was able to go home the following day.
Watch the full video to learn more about the procedure, see his imaging and review his specimen.
Don't trust an "occasional" thyroid surgeon with your goiter. This is all we do!
Interesting case of the week 1/14/2022: A thyroid goiter so large it grew into the carotid arteries, with Dr. Rashmi Roy of the Clayman Thyroid Center
We're back for another edition of Royters Goiters with the goiter guru!
This patient was told by many surgeons that they wouldn't operate on her because of how involved her goiter was with the surrounding carotid arteries.
Watch the full video to review her scans, see her specimen in the operating room and learn how we were able to successfully remove her thyroid with no complications.
Interesting case of the week 1/7/2022: Medical Tourism with Dr. Nate Walsh
. A 35-year-old woman from Japan was recently seen at our center for a symptomatic thyroid nodule. She was evaluated in Japan for difficulty swallowing and breathing. Work-up in Japan showed a large 3 cm nodule in the right half of her thyroid with solid and fluid composition. A needle biopsy did not reveal any cancer.
She was told by a surgeon and physician in Japan that she should monitor the nodule given the low chance of cancer based on the needle biopsy. Unfortunately, the lump in her thyroid was visible and continued to cause symptoms, and she ultimately decided to seek expert evaluation at our center.
our clinical visit, the ultrasound demonstrated a 3.8 cm mass in her right thyroid that basically filled the entire right half of her thyroid. Ultrasound images can be seen here. Solid (light gray) and fluid- filled (very dark areas) components are seen.
When nodules are this large and causing symptoms, surgery is necessary. Observation would only lead to surgery further down the road for a nodule that would certainly be larger.
Our young lady underwent removal of the right side of her thyroid, along with removal of the lymph nodes around and behind the thyroid. Thankfully, pathology revealed no cancer in the nodule or the lymph nodes. She was able to keep the healthy left half of her thyroid.
Her symptoms improved almost immediately. She experienced no change in voice, swallowing, or calcium control. Her physical appearance will remain unaltered except for a tiny, well- healed scar located in the lower portion of her neck. Our patient did wonderfully during and after surgery and recovered very nicely.
People traveling for the best medical care, known as medical tourism, is becoming increasingly popular. Expert and experienced evaluation, treatment, and follow-up for thyroid cancer is of critical importance. Distance should not be the deciding factor in your thyroid care.
Interesting case of the week 12/17/21: The importance of finding an expert thyroid surgeon with Dr. Rashmi Roy
We're back for another edition of Royter's Goiters! This week's patient is a 51-year-old woman from Alabama. She has been monitoring her goiter through ultrasounds since 2015 and over time her symptoms progressed in severity from constant clearing of the throat, to difficulty swallowing, to the point of needing a CPAP machine to breath at night.
She knew she needed surgery. The first surgeon she saw told her that her goiter was too large and surgery would require cracking her chest. Understandably, she was frightened by this and sought a second opinion. The second, third, and fourth surgeon she saw all agreed and said they would indeed need to crack her chest open in order to remove the goiter.
Luckily, she found us online. After reviewing all of her imagining, I assured her that I would be able to successfully remove the thyroid goiter without cracking her chest through a small incision above her collarbone.
Watch the video to learn about this patient's outcome, see her imaging and specimen after surgery, and find out what to look for when selecting a thyroid surgeon. It's the most important step on your road to being cured!
Interesting case of the week 12/10/21: Surgery to Cure Hashimoto’s Disease with Dr. Nate Walsh
A 45-year-old woman was seen at our center for symptomatic Hashimoto’s Disease. She reported excessive hair loss, cold intolerance, daytime fatigue, and insomnia. Our patient had also been frequently changing the dose of thyroid medication, but was still not feeling great. Ultrasound images of her diseased thyroid are seen below.
Figure 1: Ultrasound image of a Hashimoto’s thyroid. Note the irregular, scalloped, moth-eaten appearance of the thyroid tissue.
Due to her symptoms, the duration of her medical treatment, and her overall frustration with not feeling well, she elected to have her thyroid removed. Our young lady underwent removal of her entire thyroid (total thyroidectomy). The Hashimoto’s disease was cured as a result of her thyroid surgery. Her symptoms improved almost immediately. She experienced no change in voice, swallowing, or calcium control (parathyroid glands were healthy). Her physical appearance will remain unaltered except for a small scar located in the lower portion of her neck. Our patient did wonderfully during and after surgery and recovered very nicely.
Hashimoto’s thyroiditis, or Hashimoto’s disease, is a chronic inflammatory condition of the thyroid gland caused by an autoimmune disorder where the patient develops antibodies to thyroglobulin (a normal protein produced by the thyroid gland). Thus, the immune system attacks your own thyroid gland, causing inflammation and fibrosis/scarring of the gland. Long- standing Hashimoto’s thyroiditis is frequently associated with a diseased thyroid (secondary to inflammation and scarring). This ultimately leads to decreased thyroid hormone production (hypothyroidism) and subsequent symptoms.
Most patients who require treatment for Hashimoto’s disease do well with thyroid hormone medication and do not require surgery. A small subset of patients, however, have difficulty finding the right dosage of thyroid medication to control and improve symptoms. Additionally, some patients also continue to feel poorly or have symptoms despite being on an appropriate dose of thyroid medication. As such, a small group of patients with Hashimoto’s disease benefit tremendously from expert thyroid surgery to remove the thyroid gland. You cannot have Hashimoto’s disease without your thyroid. Therefore, complete thyroid removal cures Hashimoto’s disease.
When dealing with thyroid conditions, thyroid cancer, and thyroid surgery, skill and experience are paramount. The critical nerves of the voice box that control sensation and movement of the vocal cords must be identified and preserved in every thyroid operation. In addition, the parathyroid glands that control calcium in the body, must also be identified and spared. Only expert, high-volume surgeons should perform thyroid surgery.
Skilled and experienced evaluation, treatment, and follow-up for thyroid disease is of critical importance. Entrust only the best!
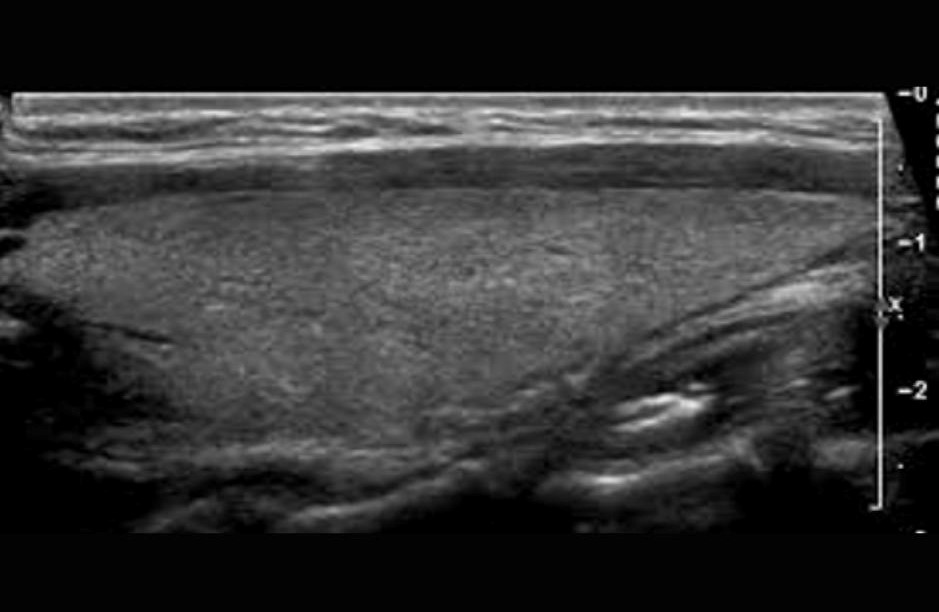
Figure 2: Ultrasound image of another patient’s normal, healthy half (lobe) of the thyroid. Note the even consistency and appearance of the tissue.
Interesting case of the week 12/3/21: "The Nerve of that Nerve" with Dr. Rashmi Roy
. We had a lovely 38 year old woman come see us from Illinois for a right sided multinodular goiter. She was healthy with no known medical or surgical history. Her physical exam was significant for masses that could be felt on the right side of her neck. Her only symptom from her nodules was trouble swallowing dry food. She was not experiencing any voice changes or trouble breathing. During her evaluation, we performed a laryngoscopy (small camera) to visualize her vocal cord movement and an ultrasound of her thyroid gland and lymph nodes. Her vocal cords were functioning normally, and her ultrasound showed several right sided thyroid nodules that looked suspicious on ultrasound. She did not have any suspicious lymph nodes seen on her preoperative ultrasound. Biopsy of her thyroid nodules were indeterminate with a 50% risk of thyroid cancer.
She was taken to the operative room that morning for removal of the right thyroid lobe and the lymph nodes behind the right thyroid lobe. This is a very standard operation at our center. When performing thyroid operations, the foundation of these surgeries is to identify and preserve the nerve that goes to the vocal cords. This nerve is called the recurrent laryngeal nerve (nerve to the voice box). Its function is to innervate the vocal cords so that we can speak with a normal voice. We cannot proceed with the operation until this nerve is located and safely preserved. There is a predictable location of this nerve on both the left and right side of the neck, and we are able to locate it very quickly. Once identified, the recurrent laryngeal nerve also has a predictable course that can be followed in order to dissect the nerve safely to the voice box.
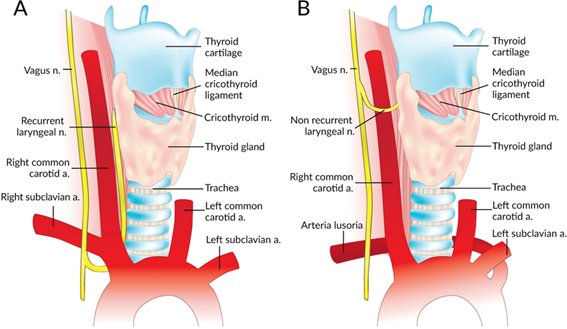
The interesting part of this case is that the nerve to the voicebox was in a very unusual location! On ONLY the right side of the neck, the laryngeal nerve can vary in its location and course <1% of the time. Only a highly experienced surgeon will be able to know the different tracts that the right laryngeal nerve can take and be able to locate it and save it. Normally the right recurrent laryngeal nerve starts at the voice box and travels DOWN the neck to wrap around the major vessels coming off of the heart. In this case, the nerve did not travel down the neck at all, but instead it travelled ACROSS the neck in a very high location. Once the nerve could not be identified in a normal location, we knew that it must be a NONrecurrent laryngeal nerve. We knew exactly where we should be looking next. We were then able to identify and save her nonrecurrent laryngeal nerve and perform the thyroidectomy successfully.
She woke up cancer free with a normal voice and was discharged to the hotel the very same day with no complications. She was very grateful that she came to the Clayman Thyroid Center for expert thyroid surgery.
Figure A: Normal right recurrent laryngeal nerve
Figure B: NONrecurrent right recurrent laryngeal nerve
Interesting case of the week 11/19/21: Enlarged Lymph Nodes in the Neck in a Young Adult with Dr. Nate Walsh
This week, a 24-year-old gentleman was seen at our center for #papillarythyroidcancer that had spread to the lymph nodes around/behind his thyroid as well as with the lymph nodes in the side of the neck on the left. The patient had noted 2 lumps in the left side of his neck for several months. Over that course of time, he underwent multiple laboratory and imaging tests for possible causes of the enlarged lymph nodes, and he was treated with antibiotics and steroids. Ultimately, a needle biopsy of one of the large lymph nodes in the left side of his neck revealed metastatic papillary thyroid cancer. CT scan and outside ultrasound, however, did not show a clearly defined cancer within the thyroid gland itself. He sought care at our center.
At our evaluation, this gentleman had multiple suspicious lymph nodes around and behind his thyroid on both sides. Additionally, he had obvious spread of thyroid cancer to the lymph nodes in the left side of his neck that accounted for the lumps he was able to feel himself. Where the thyroid cancer began, as noted in Figure 5 below, was a tiny 5 mm cancerous nodule in the left thyroid lobe. Due to his age and metastatic disease, he needed surgery followed by radioactive iodine treatment.
The patient underwent a total thyroidectomy (complete removal of the thyroid gland) combined with removal of the lymph nodes around and behind the thyroid on both sides as well as all the lymph nodes in the side compartment of his neck on the left. This is called a left modified neck dissection. Final pathology confirmed a small left papillary thyroid cancer within the thyroid gland that had spread to multiple lymph nodes in his neck. He experienced no change in voice or swallowing, calcium control (remaining parathyroid glands were healthy). His physical appearance will remain unaltered except for a scar located in the lower portion of his neck. Our patient did wonderfully during and after surgery and is recovering very nicely.
Expert and experienced evaluation, treatment, and follow-up for thyroid cancer is of paramount importance. This young gentleman had metastatic thyroid cancer that affected the lymph nodes around/behind the thyroid (that are typically not removed by most surgeons), but that also had spread to the left side of the neck. Prior to evaluation at our center, he was worked-up over the course of a couple months for suspected viral, bacterial, or infectious causes, but cancer was not a consideration for over 2 months. Young patients develop thyroid cancer as well. Persistent lymph nodes following antibiotic therapy should be appropriately evaluated. Furthermore, his papillary thyroid cancer was so small, only our expert ultrasound team was able to diagnose the primary cancerous nodule.
This case underscores the importance of healthcare providers thoroughly understanding thyroid cancer. The complete picture of the patient must always be considered. While viral causes and other illnesses often cause swollen lymph nodes, particularly in younger patients, thyroid cancer must be considered. Multiple enlarged lymph nodes, particularly if only affecting 1 side of the neck, should be biopsied promptly after diagnosis if there is no obvious infectious cause and the patient does not improve within days of medical treatment (i.e. antibiotic and/or steroids). Furthermore, this case also illustrates the fact that small or even microscopic (less than 1 cm) thyroid cancers can spread to lymph nodes in the neck.
Whenever a test or study result seems out of place, particularly after the 1-2 most common causes are ruled out, appropriate action and further investigation should be sought immediately. When an imaging study displays concerning signs of malignancy, such as irregular, enlarged lymph nodes in the side of the neck, cancer should be the diagnosis until proven otherwise. If the clinician does not know what diagnoses to look for (or what they are looking at based on imaging and labs), a small, but aggressive, thyroid cancer can be overlooked.
Figure 1: Ultrasound images demonstrating enlarged, irregular-appearing lymph nodes around/behind the left thyroid cancer. These are denoted by the blue outline.
Figure 2: Very small papillary thyroid cancer in the left side of the thyroid. Nodule is circled in blue.
Interesting case of the week 11/12/21: Massive goiter causing trachea compression to the point of near suffocation
This is a story about a patient getting very bad advice which led to a life threatening condition.
Today's patient is a young man in his 30s with a 15-year history of a mass in his thyroid. The mass was very, very large, but because of his weight it was difficult to notice.
He wasn't really experiencing any symptoms and was told time and time again by doctors that if it wasn't bothering him, it wasn't a problem. He continued to monitor it with ultrasounds.
By the time he started experiencing significant symptoms, the mass had grown into his chest and he was told by his doctors that it was too late to do anything about it. So again, he did nothing.
His symptoms got so severe that he could not walk, breath, or sleep normally. He even needed a CPAP machine when he slept because he would stop breathing due to his trachea being compressed so badly by this mass.
Continue watching the full video to see this patient in the operating room, learn about how we treated him and hear how he is doing today.
Interesting case of the week 11/3/21: Metastatic Thyroid Cancer with Benign Thyroid Biopsy: A Cautionary Tale, with Dr. Nate Walsh
This week, we'll be examining the case of a 75-year-old gentleman who was seen at our center for thyroid cancer that had spread to a bone in his right pelvis.
Interestingly, he had undergone needle biopsies of two left-sided nodules 4 years prior that demonstrated benign cells. Although the nodules were concerning on outside ultrasound examination, further molecular/genetic testing returned benign results. As a result, his thyroid cancer remained undiagnosed until the biopsy of his pelvic metastasis.
At our evaluation, this gentleman had multiple suspicious nodules in his left thyroid. See figures 1 and 2: Ultrasound images of two thyroid nodules. The blue line indicates these nodules. Both have irregular borders. These findings are concerning and should not be ignored independent of a needle biopsy or genetic testing result.
Combined with the fact that he had distant metastatic disease, he undoubtedly needed surgery and radioactive iodine treatment.
Our patient underwent a total thyroidectomy along with removal of the lymph nodes. His thyroid cancer surgery was very complex due to prior parathyroid surgery and previous radiation treatment that caused tremendous scarring. Additionally, his thyroid cancer was growing into the outer layer of the nerve to his voice box.
We were able to completely remove his cancer while sparing the nerves to the voice box. Thorough removal of the cancer is critical, as leaving cancer behind will lead to further surgery that is very difficult or not able to be performed without significant adverse side effects.
Final pathology revealed follicular variant of papillary thyroid cancer. Additionally, the lymph nodes were involved with local spread of his thyroid cancer. Our patient did great during and after surgery and is recovering nicely.
This case underscores the importance of healthcare providers thoroughly understanding thyroid cancer. An ultrasound study with concerning signs of malignancy should not be disregarded based upon a needle biopsy or genetic testing-- the entire picture must be considered.
Interesting case of the week 10/29/21: Recurrent Laryngeal Nerve with Dr. Rashmi Roy
We're back with another edition of Royter's Goiters!
This week, we have a 48-year-old woman suffering from a very large goiter due to her Graves' disease. She was managing her Graves' disease with thyroid medication and monitoring her goiter, but she was still experiencing symptoms like difficulty speaking and breathing.
She was terrified of having surgery and avoided it for as long as she possibly could. But her symptoms progressed to the point that any activity at all was causing significant shortness of breath.
During her evaluation, we of course saw a very large mass, but much more concerning were her vocal cords. The left side of her vocal cord was almost paralyzed.
Continuing watching the video to learn more about the case, join me in the operating room and hear about this patient's outcome.
Interesting case of the week 10/22/21: When medical management fails Graves’ Disease patients with Dr. Rashmi Roy
We’re back for another edition of Royter’s Goiters!
This week I saw a patient who was diagnosed with #GravesDisease several years ago. She was trying to manage her disease with several medications, none of which were working for her. While trying these medications, her thyroid grew substantially and she developed a large #GravesGoiter in her neck as well as Graves’ eye disease. Because her goiter was so large, she was suffering significant symptoms including difficulty breathing, swallowing and speaking.
I removed her thyroid gland with an operation that lasted about an hour. She spent some time in recovery and was discharged the following day without any complications.
Watch the full video to hear me discuss this case in detail, review her imaging and show you the specimen I removed.
If you have Graves’ Disease and you’re failing medical management, please consider surgery. It’s the best option for your recovery.
Interesting case of the week 10/15/21: Underdiagnosed Aggressive Papillary Thyroid Cancer in Multiple Locations With Dr. Nate Walsh
A 66-year-old gentleman was seen at our center for a papillary thyroid cancer. Ultrasound done at another facility also noted a nodule in the isthmus. He was seen at our center for further evaluation.
During our evaluation, a very thorough ultrasound was done. This confirmed that the nodule in the isthmus was also a thyroid cancer. Additionally, he had 2 other nodules suggestive of thyroid cancer in the left side of his thyroid gland. Suspicious lymph nodes near the right thyroid and one in the right side of the neck, not noted previously, were also discovered. Due to our findings, this gentleman was scheduled for complete removal of his thyroid along with the lymph nodes around the thyroid on both sides.
As you can see in the images below, the calcifications, irregular border, increased blood flow (dots of red-orange), and inconsistent appearance of these nodules indicate thyroid cancer until proven otherwise. In these first two images, the arrows and red line indicate areas of calcification and irregular or not well-defined borders for this cancerous tumor. The arrows in this third image above show increased areas of blood flow in the thyroid cancer (red-orange areas), calcifications that create shadowing, and the lack of a border on the bottom of the thyroid cancer.
Our patient underwent a total thyroidectomy along with removal of the lymph nodes around the thyroid on both sides. His surgery was very tedious and complicated due to the cancer growing into the outer layer of the nerve to his voice box. We were able to completely remove his cancer while sparing the nerve to the voice box.
Complete removal of the cancer is critical, as leaving any cancer behind will lead to further surgery that is very difficult or not able to be performed without significant adverse side effects. Fortunately for him, we did not have to remove part of the nerve to the voice box, and he had an excellent outcome.

Interesting case of the week 10/8/21: Metastatic Papillary Thyroid Cancer and Hyperparathyroidism with Dr. Rashmi Roy
Mrs. P is a 54 year-old lovely woman who was being evaluated in Virginia for bone pain. She is an otherwise healthy woman, with past medical history only significant for hypertension, for which she was taking lisinopril and hydrochlorathiazide. Her bone pain was chalked up to arthritis and was asked to get an MRI.
As part of her evaluation, she also had routine bloodwork done which showed abnormal thyroid function tests and a high calcium level. Her doctor attributed her high calcium levels to her hydrochlorothiazide, but they did obtain a thyroid ultrasound for her abnormal thyroid function tests. Her ultrasound showed a suspicious right sided thyroid nodule and a suspicious right lateral neck lymph node. These were both biopsied confirming papillary thyroid cancer with metastasis to her right lateral neck lymph node. Once she was given this diagnosis, she found us online and filled out a form to become our patient.
During our evaluation, we performed a high-resolution ultrasound to look at her thyroid gland and her lymph nodes on both sides of her neck. Our ultrasound confirmed the presence of multiple lymph nodes in her right lateral neck with metastatic thyroid cancer. Most importantly, her bone pain and elevated calcium levels were a red flag for us, and we obtained a PTH level. With an elevated PTH level and elevated calcium level, we diagnosed her with hyperparathyroidism. Fortunately, she came to see us so that we could diagnose her properly and cure both her hyperparathyroidism and thyroid cancer in the SAME operation.
This lovely woman underwent a successful total thyroidectomy, bilateral central neck dissection, right lateral neck dissection, and parathyroidectomy. She tolerated the procedure beautifully and was discharged the following day with a well healing incision and feeling great. She is back home in Virginia enjoying her daily bike rides, feeling amazing with a normal voice, NO MORE bone pain or achy muscles, and CANCER FREE!!
