Substernal Goiter: Diagnosis and Treatment of Substernal Goiter
What is a Substernal Goiter?
A substernal goiter is a condition where there is an abnormal enlargement of your thyroid gland that extends into the chest. There are many reported definitions of the condition, and the most commonly accepted definition is as follows: when >50% of the volume of a goiter extends into the chest. Most thyroid goiters do not produce any pain, but they may produce symptoms due to their size itself. The most common symptom from a thyroid goiter is a lump or mass in the neck. However, substernal goiters may not produce a lump in the neck because they may not grow outward. Their symptoms are often late in development until they produce pressure from the lack of ability of the sternum to allow expansion of the goiter. The goiter may actually grow inwards toward the back portion of your neck and down into the chest area. Other symptoms from a substernal goiter may include a sense of a lump in the throat, difficulty swallowing, difficulty breathing and even in extreme cases, voice changes and even vocal cord paralysis. (F. M. deSouza and P. E. Smith, “Retrosternal goiter,” The Journal of Otolaryngology, vol. 12, no. 6, pp. 393–396, 1983.)
The most common cause of substernal goiters are long standing multinodular goiters that have grown over many, many years into the chest cavity. The incidence of substernal goiters among patients with thyroid goiters is reported to range from approximately 5-15%. (Y. S. Lin, H. Y. Wu, C. W. Lee, C. C. Hsu, T. C. Chao, and M. C. Yu, “Surgical management of substernal goitres at a tertiary referral centre: a retrospective cohort study of 2,104 patients,” International Journal of Surgery, vol. 27, pp. 46–52, 2016.)
Goiter Guru on YouTube
Dr. Rashmi Roy, Senior Surgeon at the Clayman Thyroid Center & Hospital for Endorine Surgery, has an entire YouTube channel dedicated to thyroid goiters. Dr. Roy operates on a significant number of patients with thyroid goiters, many of whom other surgeons refuse because of their complexities. Check out the Goiter Guru YouTube Channel here.Symptoms of substernal/retrosternal goiters
The thyroid sits on top of the trachea (windpipe) and esophagus (swallowing tube). Due to the size and location of substernal goiters, they likely will produce some compressive symptoms. However, approximately 15-50% of patients have no symptoms whatsoever. When encountered, the most common symptoms associated with substernal goiter are:
- difficulty breathing
- stridor
- hoarseness
- cough
- wheezing
- presence of a bothersome cervical mass.
- difficulty swallowing (feeling like something needs to be swallowed but does not move)
- Pemberton’s sign (trouble breathing, stridor, facial flushing in certain positions)
These symptoms do not differ greatly from those of patients with cervical (neck) goiters, but they may be more severe because of the presence of the mass within the bony chest cavity. Usually respiratory symptoms are more common, but difficulty swallowing can occur in up to one third of patients. (White, M.L., Doherty, G.M. & Gauger, P.G. Evidence-Based Surgical Management of Substernal Goiter. World J Surg 32, 1285–1300, 2008).
In the 1940’s, Dr. Hugh Pemberton drew attention to the positional nature of these symptoms in some patients with a substernal goiter. Some patients will complain of trouble breathing, stridor, or facial flushing only when they are laying down flat, when their arms are raised or when their neck is extended, or when they are looking to the right or the left. This occurs as a result of the thyroid goiter being drawn into the bony chest cavity. (MR Katlic, C Wang, HC Grillo – Substernal Goiter. The Annals of thoracic surgery, 1985)
Become Our Patient
Founded by Dr Gary Clayman, the Clayman Thyroid Center is widely known as America’s leading thyroid surgery center performing nearly 2000 thyroid operations annually. Our reputation as the best thyroid surgeons means patients from all over the US and many foreign countries travel to Tampa for their thyroid surgery. With same-day evaluation and surgery scheduling, we make traveling for thyroid surgery convenient for every patient.What Is The Evaluation Of A Substernal Goiter?
The following are a list of tests that are required in the evaluation of a patient with a Substernal Goiter.
Evaluation of a Substernal Goiter Patient:
- Complete Medical History and Physical Examination
- Ultrasound
- High resolution CAT scan with contrast from skull base to below the branching of your trachea in your chest
- Blood Tests
- TSH
- T3 and T4
- Thyroglobulin (we obtain but not all doctors do so)
- Thyroglobulin Antibody (we obtain because it lets us know if there is an underlying inflammatory condition of the thyroid)
- Thyroid Stimulating Immunoglobulin
- Laryngoscopy (looking at the voice box)
- Ultrasound with possible Fine Needle Aspiration guided (FNA) may be indicated based upon findings (routinely, needle biopsy is not required in order to determine whether a surgery is indicated!) However, large goiters can hide the potential of thyroid cancers. Therefore comprehensive evaluation of neck lymph nodes should be performed on all substernal thyroid patients. Lymph nodes of concern should be biopsied if found on comprehensive evaluation.
Medical history and physical examination is required for all patients with a substernal goiter. If there is a suspicion that you may have a substernal goiter, your health care professional will want to know your complete medical history. You will be asked questions about your possible risk factors, symptoms, and any other health problems or concerns. If someone in your family has had a diagnosis of thyroid goiter, thyroid cancer or other endocrine cancers, these are important factors to discuss with your doctor.
Your doctor will examine you to get more information about possible signs of thyroid goiter and other health problems. During the exam, the doctor will pay special attention to the size and firmness of your thyroid and any enlarged lymph nodes in your neck. Examination of your voice box is part of the physical examination obtained by the surgeon for any thyroid goiter. A small lighted microscope is used to look at the voice box to determine how the vocal cords of the voice box are functioning. Even though a patient does not report change in their voice does not insure that the vocal cords are working normally. A vocal cord that is paralyzed greatly increases the concern that a thyroid goiter may be hiding a thyroid cancer.
Substernal Goiter: The Definitive Diagnosis of a Substernal/Retrosternal Goiter is Made by High Resolution Ultrasound Examination
- The diagnosis of a substernal goiter is made with a comprehensive ultrasound examination of the entire thyroid gland and neck lymph nodes. Ultrasound exposes you to no radiation whatsoever. It uses sound waves to look beneath the skin at the important structures of your neck. Needle biopsy is only indicated if there is a mass within the thyroid goiter which is suspicious for malignancy or abnormal lymph nodes in your neck are identified.
- Ultrasound is used to see the thyroid gland and the lymph node of the neck. During biopsy, the ultrasound helps make sure they are getting FNA samples from the right areas.
- If the whole thyroid is not being surgically removed, FNA is generally done on all thyroid nodules that are big enough to be felt or are of concern. This means that they are larger than about 1 centimeter (about 1/2 inch) across.
- FNA biopsies of swollen or abnormal appearing lymph nodes in the neck may be more informative than the thyroid nodule itself in obtaining a diagnosis of a thyroid cancer.
- Cells from the suspicious area are removed without an incision or discomfort and looked at under a microscope.
- The process of obtaining this small sampling of cells is called fine needle aspiration (FNA) cytology.
- This type of biopsy can usually be done in your doctor's office or clinic.
- Before the biopsy, local anesthesia (numbing medicine) may be injected into the skin over the thyroid nodule.
- Your doctor will place a thin, hollow needle directly into any suspicious dominant nodules within the thyroid goiter to aspirate (take out) some cells and possibly a few drops of fluid into a syringe.
- The doctor usually repeats this 2 or 3 more times, taking samples from several areas of the nodule.
- The content of the needle and syringe are then placed on a glass slide and then the FNA samples are then sent to a lab, where they are looked at under a microscope by the expert Cytologist (Doctor that examines cells) to see if the cells look cancerous or benign.
- Cytology means looking at just the cells under the microscope.
- Thyroid cytology requires an expert physician (called a Cytologist) trained specifically in the diagnosis of thyroid nodules and thyroid cancers!!!
- Unfortunately, the diagnosis of thyroid nodules are frequently misinterpreted by unskilled or inexperienced Cytologists. Bleeding at the biopsy site is very rare except in people with bleeding disorders. Even when this occurs, the bleeding is almost always very self-limited. Be sure to tell your doctor if you have problems with bleeding or are taking medicines that could affect bleeding, such as aspirin or blood thinners.
- Sometimes an FNA biopsy will need to be repeated because the samples didn't contain enough cells.
- Most FNA biopsies will show that the thyroid goiters are benign.
- Rarely, the FNA biopsy may come back as benign even though a diagnosis of a thyroid cancer is actually present.
Substernal Goiter: When is a Radioiodine Scan Ordered?
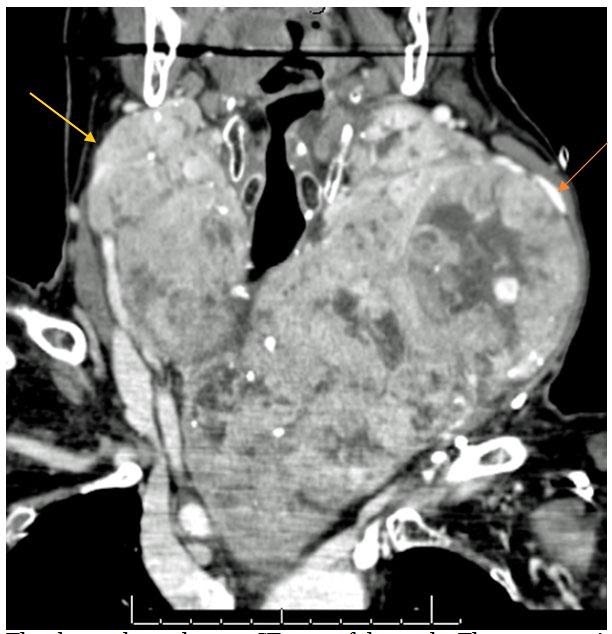 The above photo shows a CT scan of the neck. The arrows point to a thyroid goiter that essentially fills the entire neck and extends into the upper chest surrounded by the blood vessels leaving the heart and veins leading the return of blood to the heart. This requires a straight forward surgery with a lower neck collar incision and leaving the hospital the very next morning.
The above photo shows a CT scan of the neck. The arrows point to a thyroid goiter that essentially fills the entire neck and extends into the upper chest surrounded by the blood vessels leaving the heart and veins leading the return of blood to the heart. This requires a straight forward surgery with a lower neck collar incision and leaving the hospital the very next morning.
If you have a thyroid goiter and your blood tests also demonstrate that your thyroid hormone level is too high (hyperthyroidism), this is the only instance that a radioiodine scan (thyroid scan) is indicated. In these cases, the thyroid stimulating hormone (TSH) will be very low and in cases of Grave's disease, the thyroid stimulating immunoglobulin will be very high. The thyroid goiter patient may or may not have recognized symptoms of their hyperthyroidism.
During the thyroid scan, the patient will be given a small amount of radioactive iodine in a pill and a special imaging camera is utilized to determine how much iodine is taken up by the thyroid gland and if the thyroid goiter takes up iodine throughout the thyroid gland or whether there is a single "hot" area in the thyroid , relative to the remainder of the thyroid gland (this is called a "hot nodule"). If a thyroid nodule has less iodine uptake than the rest of the thyroid gland, then the thyroid nodule is called a "cold nodule". In patients with multinodular goiter, frequently several of the nodules of the thyroid will be cystic and filled with fluid. These cystic areas of a multinodular goiter are expected to take up less iodine than the rest of the gland and appear "cold".
Hot nodules are almost always non-cancerous but the preferred management of hot nodules is frequently surgery since it is a clear, safe and 100% effective therapy for the hyperthyroidism.
Substernal Goiter: Should a CT Scan ordered?
With a substernal goiter, physical examination and or ultrasound cannot completely determine how far the goiter actually goes. Therefore, a CT scan should be ordered. The CT scan will show areas that the thyroid goiter extends and prepare the expert thyroid surgeon their safe and effective approach to remove all of the goiter gland and spare all other structures. In rare circumstances, portions of the thyroid gland will be separated from the main thyroid goiter and a CAT scan may be the only way to know that there is another mass behind the chest wall which may need to be removed as well. Without this information, an incomplete operation could potentially occur. For that reason, all substernal goiters require a CAT scan as imaging.
Surgical Treatment For Substernal Goiters?
Substernal thyroid goiters clearly need surgical management. Indications of removal include:
- The thyroid goiter is large (producing a visible mass in the neck)
- The thyroid goiter is producing symptoms on the breathing tube or swallowing tube
- The thyroid goiter is producing excessive thyroid hormone
- Thyroid nodules which have Indeterminate or suspicious for cancer FNAs.
- Multinodular goiters producing symptoms
- A thyroid goiter which has progressed or remains symptomatic following RAI treatment
Even though a substernal goiter may extend extensively below the sternum (breast bone) and go well into the chest, these goiters can almost routinely be removed through a relatively straight forward low collar incision in the lower neck. These operations should not be performed by occasional thyroid surgeons. Only expert thyroid surgeons should be doing this operations. Incomplete removal of the thyroid and complications in preserving all of the critical structures beneath and around the thyroid gland are frequent events among inexperienced and occasional thyroid surgeons. If your surgeon is telling you that they need to "split your chest" or "open your sternum", make sure that you have identified a highly experience thyroid surgeon. Seek an expert second opinion. Opening of the chest in the surgical management of substernal goiter is almost never actually required.