Hashimoto’s Thyroiditis
- Most common cause of hypothyroidism in the United States
- Also known as chronic lymphocytic thyroiditis or autoimmune thyroiditis
- An autoimmune condition
- Diagnosed by low TSH and detection of anti-thyroid antibodies
- Effects women more common than men
- Often appears between 40-60 years of age
- Appears to have some hereditary component
- Increased risk if you have other autoimmune disorders
- Can produce pseudonodules
What Are The Symptoms of Hashimoto’s Thyroiditis?
Early in the course of the disease, symptoms may not appear because the condition progresses slowly. However, over time symptoms arise.
The following are a list of the more common symptoms of Hashimoto’s Thyroiditis:
- Large thyroid or goiter
- Neck/thyroid tenderness
- Fatigue
- Weight gain
- Cold intolerance
- Joint/muscle pain
- Constipation
- Irregular menstrual periods
- Dry/thinning hair
- Depression
- Memory problems
- Slowed heart rate
What Causes Hashimoto’s Thyroiditis?
Hashimoto’s thyroiditis is an autoimmune disease where the immune system malfunctions. We do not know exactly why it occurs, but we think it is multifactorial. Excessive iodine may trigger thyroid disease. There is likely a hormonal component because women are affected much more commonly than men. Lastly, there is likely a genetic component because Hashimoto’s thyroiditis runs in families who have thyroid disease or autoimmune diseases. Some anecdotal evidence suggests that dietary gluten may contribute to Hashimoto’s thyroiditis and dietary changes may improve some symptoms.
Regardless of the cause, we know that the immune system is finding our thyroid gland abnormal and mounts an antibody attack against the gland. Instead of the immune system protecting the body, the immune system makes antibodies that attack the thyroid gland. A large number of lymphocytes or white blood cells, that are part of the immune system, build up in the thyroid and produce antibodies. These antibodies are anti-thyroid antibodies that are more specifically called thyroid peroxidase antibodies and the anti-thyroglobulin antibodies.
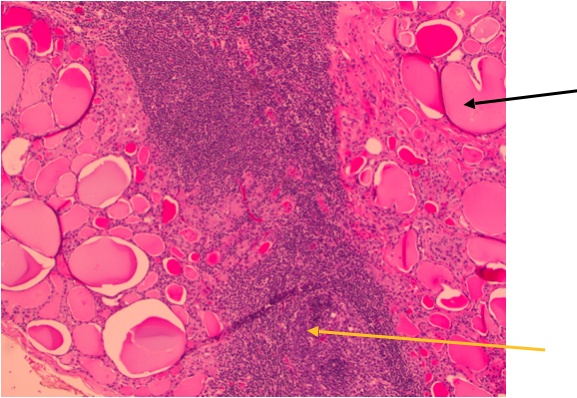
This is a picture of a pathology slide of a patient that underwent thyroid cancer surgery and Hashimoto’s thyroiditis was also present. Thyroid cancer and Hashimoto’s thyroiditis are not exclusive of each other. The black arrow points to thyroid tissue. The large pink areas are called thyroid follicles. The yellow arrow points to dark purple cells in the thyroid gland. These are the bodies white blood cells. They are not normally present in the thyroid gland in large numbers except in thyroiditis or inflammation.
Hashimoto’s Thyroiditis Diagnosis: How is it made?
The following are a list of tests that are required in the evaluation of a patient with Hashimoto’s thyroiditis:
- Complete Medical History and Physical Examination
- Ultrasound
- Blood tests
- TSH
- T3 and T4
- Thyroglobulin (we obtain but not all doctors do)
- Thyroglobulin Antibody
- Thyroid Peroxidase Antibody
- Laryngoscopy (looking at voice box)
- Ultrasound with possible FNA (fine needle aspiration) biopsy
Medical History and Physical Examination is required for all patients with a potential diagnosis of Hashimoto’s thyroiditis.
If there is a suspicion that you may have a Hashimoto’s thyroiditis, your health care professional will want to know your complete medical history. You will be asked questions about your possible risk factors, symptoms, and any other health problems or concerns. If someone in your family has had a diagnosis of Hashimoto’s thyroiditis or other autoimmune disorders, these are important factors.
Your doctor will examine you to get more information about possible signs of thyroid goiter and other health problems. During the exam, the doctor will pay special attention to the size and firmness of your thyroid and any enlarged lymph nodes in your neck. Examination of your voice box is part of the physical examination obtained by the surgeon for any patient with Hashimoto’s thyroiditis. A small lighted microscope is used to look at the voice box to determine how the vocal cords of the voice box are functioning. Even though a patient does not report change in their voice does not insure that the vocal cords are working normally. Thyroid cancer must be ruled out if a vocal cord that is paralyzed. Patients do not always report changes in voice when a vocal cord has become paralyzed slowly over time.
Hashimoto’s Thyroiditis: How is diagnosis made?
- The diagnosis of Hashimoto’s thyroiditis is made with a comprehensive analysis of the blood including thyroid stimulating hormone (TSH), Free T4 levels and Free T3 levels. In Hashimoto’s thyroiditis, the TSH level can be quite high consistent with a hypothyroid condition. When the thyroid gland is not producing enough thyroid hormone (Free T4), the pituitary gland which secretes TSH is stimulated to secrete more TSH to try to increase production of thyroid hormone. But this mechanism is failing to control the hypothyroidism.
- The diagnosis of Hashimoto’s thyroiditis is made with the detection of a high TSH, low Free T4, and anti-thyroid antibodies. Hashimoto’s thyroiditis is supported by a blood test for Thyroid Peroxidase Antibodies (TPO) or Thyroglobulin Antibody. Ultrasound is used to see the thyroid gland and the lymph nodes of the neck. In Hashimoto’s thyroiditis, diffuse vascularity can be seen. Also, pseudo nodules can be seen, which are not real thyroid nodules. Pseudo nodules are an ultrasound artifact. The inflammation of Hashimotos’ thyroiditis makes the thyroid look lumpy bumpy on ultrasound. Pseudo nodules are diagnosed when the apparent nodules disappears on follow up ultrasounds. Ultrasound exposes you to no radiation whatsoever. It uses sound waves to look beneath the skin at the important structures of your neck. Needle biopsy is only indicated if there is a mass within the thyroid which is suspicious for thyroid cancer. Find out more about ultrasound evaluation and how important it is in the evaluation of thyroid cancer here: Ultrasound and evaluation of thyroid cancer.
- FNA is generally done on all thyroid nodules that are big enough to be felt. This means that they are larger than about 1 centimeter (about 1/2 inch) across.
- FNA biopsies of swollen or abnormal appearing lymph nodes in the neck may be more informative than the thyroid nodule itself in obtaining a diagnosis of thyroid cancer.
- Cells from the suspicious area are removed without an incision or discomfort and looked at under a microscope.
- The process of obtaining this small sampling of cells is called fine needle aspiration (FNA) cytology.
- This type of biopsy can usually be done in your doctor's office or clinic.
- Before the biopsy, local anesthesia (numbing medicine) may be injected into the skin over the thyroid nodule.
- Your doctor will place a thin, hollow needle directly into any suspicious dominant nodules within the thyroid goiter to aspirate (take out) some cells and possibly a few drops of fluid into a syringe.
- The doctor usually repeats this 2 or 3 more times, taking samples from several areas of the nodule.
- The content of the needle and syringe are then placed on a glass slide and then the FNA samples are then sent to a lab, where they are looked at under a microscope by the expert Cytologist to see if the cells look cancerous or benign.
- Cytology means looking at just the cells under the microscope.
- Thyroid cytology requires an expert physician (called a Cytologist) trained specifically in the diagnosis of thyroid nodules and thyroid cancers!
- Unfortunately, the diagnosis of thyroid nodules are frequently misinterpreted by unskilled or inexperienced Cytologists.
- Bleeding at the biopsy site is very rare except in people with bleeding disorders. Even when this occurs, the bleeding is almost always very self-limited. Be sure to tell your doctor if you have problems with bleeding or are taking medicines that could affect bleeding, such as aspirin or blood thinners.
- FNA biopsy sometimes need to be repeated because the samples didn't contain enough cells.
- Most thyroid nodules in Hashimoto’s thyroiditis are benign. Rarely, the FNA biopsy may come back as benign even though a diagnosis of a thyroid cancer is actually present.
Ultrasound Appearance of Hashimoto’s Thyroiditis
Hashimoto’s thyroiditis appears as a diffusely irregular gland with increased vascularity (new blood vessel flow) throughout the gland. Pseudo nodules of thyroiditis appear like well-defined nodules however they resolve over short periods of time and the diagnosis is made when the nodule can no longer be identified. Pseudonodules are not real nodules. They are an ultrasound "artifact" produced by edema (swelling) in an area of the thyroid gland. Thyroid cancer and Hashimoto’s thyroiditis are not exclusive of each other. They may co-exist together and therefore any suspicious thyroid nodule within Hashimoto’s thyroiditis should be biopsied based upon its size and overall concern. Hashimoto’s thyroiditis is commonly associated with increased size and prominence of the lymph nodes in the area of the thyroid gland. These lymph nodes cannot be differentiated from thyroid cancer lymph nodes based upon their general ultrasound appearance.
Find out more about Thyroid Cancer and spread to lymph nodes here: Thyroid Cancer Overview
Hashimoto’s Thyroiditis Ultrasound Images
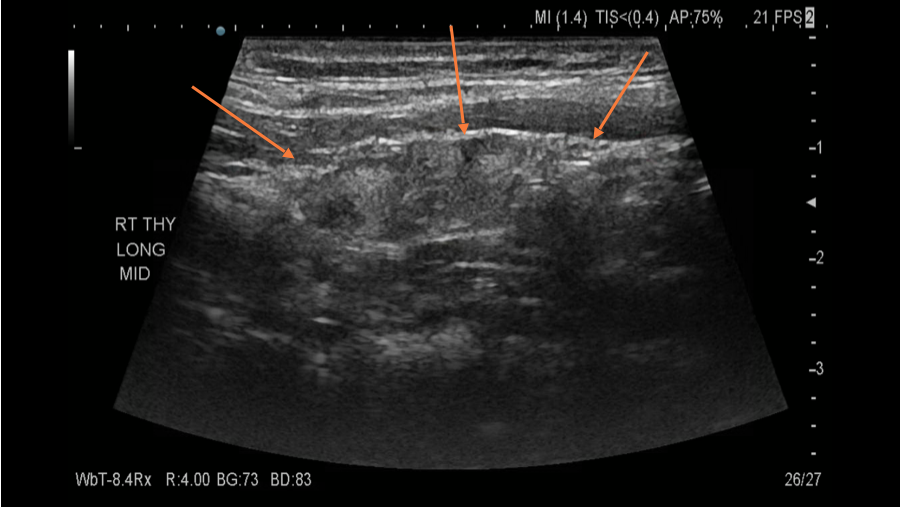
The orange arrows point to the thyroid gland. Although the patient was referred to us with a diagnosis of concerning thyroid nodules, her ultrasound revealed diffuse thyroiditis without evidence of any nodules. Therefore the prior nodules found on ultrasound were in fact "pseudo nodules".
What is the treatment for Hashimoto’s Thyroiditis?
Thyroid Hormone ReplacementYour doctor will likely prescribe you a medication to control your hypothyroidism. Thyroid hormone replacement therapy is highly effective, and likely the only treatment you will need. Thyroid hormone replacement treats this condition by compensating for the lack of hormones that the thyroid is actually producing. This medication should be prescribed by your endocrinologist who understands Hashimoto’s disease and how the medication will work. It will usually take several weeks to work.
Anti-inflammatory approachesWhen the inflammatory condition is very severe, some doctors consider a short duration of steroid therapy. Alternative medical approaches such as gluten free and avoidance of food coloring in exacerbation of Hashimoto’s disease has been advocated as well.
Thyroid SurgeryThyroid Surgery may play a role in the management of patients with Hashimoto's thyroiditis:
Thyroid Surgery may be recommended if there is:
- symptomatic thyroiditis
- thyroid enlargement and producing symptoms from its size
- mood or hormonal dysfunction. A recent randonmized controlled study suggests that surgery tremendously benefits some patients with chronic hashimoto's thyroiditis. In this study, those patients randomized to surgery did significantly better in quality of life measures than those patients managed conservatively with hormonal replacement only. They measured chronic fatigue improvement as well as General Health measures. Both were tremendously improved among surgery patients as compared to hormone replaced only patients. Published in the Annals of Internal Medicine April 2019
- A thyroid nodule is present and an FNA is suspicious for thyroid cancer
- The inflammatory condition has exhausted medical management and causing tenderness and pain in the neck or referred pain to the surrounding area. This is a rare event.
- Hashimoto’s thyroiditis surgery should only be performed by highly expert thyroid surgeons. An occasional thyroid surgeon should not do this surgery.
- Lifelong thyroid hormone replacement medication is almost certainly needed after thyroid surgery when Hashimoto’s disease is present.