Thyroid Cancer Surgery Videos
Thyroid Cancer Surgery Videos
All these surgeries are performed and narrated by Dr. Gary Clayman. Dr. Clayman performs approximately 750 thyroid cancer surgeries per year and has done so for over 27 years. All of these videos are very high definition videos so that you can see how both beautiful and delicate the structures are that are being spared while the thyroid cancer surgery is being performed. The main learning points are presented in each video.
Thyroid Lobectomy (see video)
Thyroid lobectomy is one of the most common thyroid cancer surgeries and can be appropriate for many thyroid cancers as well as non-cancerous lesions of the thyroid gland such as solitary nodules or a single thyroid nodule that is producing too much thyroid hormone. This video shows a thyroid lobectomy. The critical voice box nerves for movement and sensation are visualized and spared. The two parathyroid glands laying in close proximity to the thyroid gland are identified and preserved as well. Lymph nodes around and beneath the thyroid gland are exposed and inspected. The incision just needs to be able to allow the size of the thyroid and associated masses to be removed without them breaking or spilling. In most instances, a thyroid lobectomy is a minimally invasive surgery with a midline incision length of about one inch.
Total Thyroidectomy (see video)
In this thyroid cancer surgery, the entire thyroid gland is removed. This is the preferred thyroid cancer surgery for many thyroid cancers. If almost any thyroid cancer has spread to lymph nodes, the preferred thyroid cancer surgery is a total thyroidectomy. A small incision in the lower central neck is required which is a little more than an inch in length unless the thyroid mass or the thyroid itself requires a longer length to allow them to be “delivered”. The length of a total thyroidectomy incision is no longer than an incision for a thyroid lobectomy. All of the critical structures on both sides of the thyroid are visualized and maintained including all four parathyroid glands and all four nerves that provide movement (recurrent laryngeal nerves) and sensation and tightening to the voice box (superior laryngeal nerves). The lymph nodes along the side and beneath the thyroid gland are also examined during this surgery to make sure that they are not cancerous as well.
Left Thyroid Lobectomy converted to a Total Thyroidectomy because of findings discovered during the surgery (see video)
This is a 34 year old woman from Austin, Texas with a small papillary thyroid cancer of the left thyroid lobe. In fact, two of her direct family members are endocrinologists. Her ultrasound does not reveal any evidence of abnormal central or lateral neck lymph nodes. She desires a thyroid lobectomy if operative findings suggest that is complete surgery for her. During surgery, I identify a tiny lymph node underneath her thyroid gland that appears abnormal. Pathology at the time of surgery confirms that the lymph node contains papillary thyroid cancer. Because of the findings that her cancer had spread to lymph nodes, her surgery is then changed to a total thyroidectomy and central compartment dissection. Her pathology reveals 4 of 11 lymph nodes positive for papillary thyroid cancer. She is both ultrasound and biochemically (no stimulated evidence of thyroglobulin) cured of her thyroid cancer.
Complicated Total Thyroidectomy (see video)
A 57 year old accounting firm executive from southern Florida presents with a right sided thyroid mass. She has fine needle aspiration confirmed spread of poorly differentiated thyroid cancer to the lymph nodes of her right lateral neck. Examination of her voice box showed that both of her vocal cords of her voice box were functioning normally. During her surgery, her lymph nodes of the right central compartment (along the breathing tube and swallowing tube) have grown into her nerve of the right side of her voice box even though it was functioning normally before surgery. The correct surgery requires removing all of the cancer!!! It also requires making absolutely certainly that the other nerve to the voice box will function normally even though there is cancer along this nerve as well. Finding the voice box nerve invaded by thyroid cancer with the voice box functioning normally is very very very rare!!! Do not be concerned over this!!!! I have seen this only twice in over four thousand such surgeries with lymph nodes close to the nerve. Her voice box nerve (recurrent laryngeal nerve) is reconstructed (put back together) during surgery. She received radiation therapy has excellent normal voice and her cancer has never recurred over the past five years. You can learn a tremendous amount from watching this video.
Central Compartment Neck Dissection and Completion Thyroidectomy for Persistent Thyroid Cancer (see video)
A fifty-eight year old female attorney from North Carolina who had another surgeon perform a “total thyroidectomy and bilateral paratracheal dissection (central compartment dissection) three years ago. Her thyroglobulin (marker of her thyroid cancer) continued to rise and nodules on her ultrasound were detected and growing following this first surgery. The surgeon told the patient and her husband that they left thyroid tissue on the left side near the nerve. (This is a critical error of less experienced thyroid surgeons and places the patient at grave risk for cancer to grow into the breathing tube.) She received radioactive iodine on two different occasions with iodine going to the central area of the neck only with the first treatment. She presents to me with biopsy positive disease on both the right and left sides of the breathing tube (bilateral central compartment involvement). See in the video the difference in appearance and ease of removing lymph nodes with recurrent or persistent thyroid cancer as compared to remaining thyroid tissue. This surgery should only be performed by the most experienced thyroid cancer surgeons. She completely recovered from the surgery with normal voice box function and calcium control (parathyroid function). She received no other treatment and her chance of this coming back in her neck is less than 2%.
Modified Neck Dissection (anterolateral neck dissection) for Thyroid Cancer (see video)
The modified neck dissection (anterolateral neck dissection) for thyroid cancer is, in fact, a beautiful surgery which spares all major blood vessels, nerves, and muscles and basically only removes lymph nodes and some fatty tissue. The modified neck dissection does not change due to the type of thyroid cancer. Therefor the thyroid cancer surgery neck dissection is the same for any type of thyroid cancer if ultrasound or CAT scans show spread of cancer to the lateral neck lymph nodes. The lymph nodes removed are those which are at risk of containing the spread of thyroid cancer. These at risk lymph nodes are quite predictable. The upper neck lymph nodes are level II, the middle neck level III, the lower neck level IV, and the most furthest away from the thyroid gland, level V. It is very rare for critical structures to be involved in the neck. The CAT scan obtained before surgery examines the location of the spread of cancer and helps guide the surgery.
There are some differences between the left modified neck dissection and the right modified neck dissection. One vessel that carries fat from the abdomen, through the chest and then into the neck is most commonly found in the left lower neck. It is called the thoracic duct. Unfortunately, thyroid cancer can frequently spread to the lymph nodes surrounding the thoracic duct, therefore this fat carrying vessel must be tied off so it does not leak fatty fluid into the neck called chyle. But anatomy can sometimes fool you and these fat carrying vessels may be found also sometimes in the right neck and central compartment as well.
See a left modified neck dissection and compare it yourself to the right modified neck dissection.
The incisions are only in the lower neck immediately above the collar bone and see for yourself how normal the neck looks and functions following surgery.
Thyroid Cancer Surgery: Identifying and Sparing the Nerves to the Voice Box (Recurrent laryngeal nerves [rln]!
There are, in fact, two important nerves to the voice box on each side of the thyroid that must be identified and spared. One is called the external branch of the superior laryngeal nerve and the second is the recurrent laryngeal nerve. Both of these nerves are important. Both of these nerves need to be visualized and preserved (unless grossly invaded by thyroid cancer….which is very very rare!!!!). Most importantly, although nerve monitoring is not harmful in basically any way, it does not help spare or in fact help in the identification of the nerves to the voice box. If your surgeon says or needs nerve monitoring to find the nerves to the voice box, find yourself another thyroid cancer surgeon.
[TODO: Insert video of recurrent laryngeal nerves here.]
Here is a video showing how both beautiful and fine the recurrent laryngeal nerves to the voice box appear during a surgery. Notice the fine tiny branches to the nerve. This high definition video is about five times magnification. This is the same as the special glasses that I routinely wear in all thyroid cancer surgery. You are seeing exactly what I see every day. If your surgeon can’t see this or do this, find another surgeon to do your thyroid cancer surgery.
The recurrent laryngeal nerves produce all the major and fine movements of the vocal cords. They produce the movements that produce all voice and singing. But the other function of the recurrent laryngeal nerves are to provide all the movement of the vocal cords in maximal opening of the voice box for taking air into the lungs. Don’t forget there are the ABC’s of living. Airway, breathing and circulation. The recurrent laryngeal nerves control airway!!!
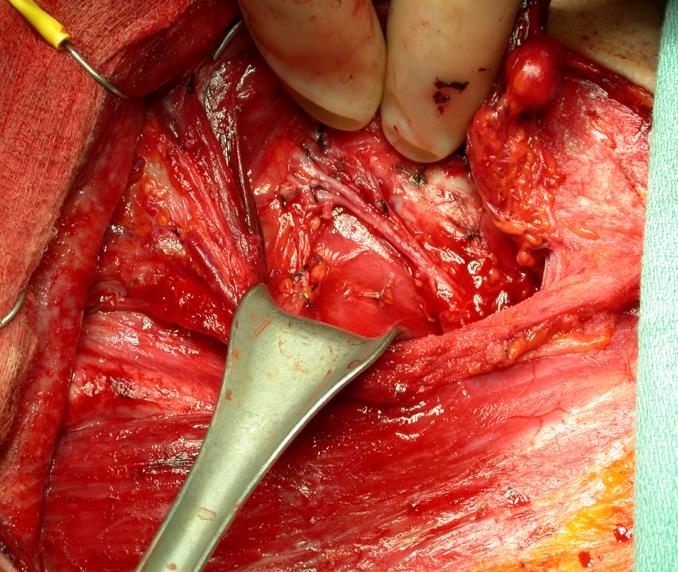

Here is a picture of a right recurrent laryngeal nerve. Lymph nodes with cancer surrounding the nerve does not mean the nerve needs to be removed. It means that all of the branches of the nerve need to be followed and saved and only the lymph nodes removed. The picture to the left shows the lymph nodes in front have been removed but the ones behind remain. The picture to the right shows that all of the small branches of the nerve have been spared and all the thyroid cancer has been removed. The arrows point to five of the major branches of the right recurrent laryngeal in this patient who had lymph nodes completely surrounding her nerve. It only takes a couple of minutes but means everything to the patient’s vocal cord function and control of their thyroid cancer.
Damage to the vocal cord nerves can produce drastic or minor changes to the quality of voice. Importantly, losing one vocal cord nerve can cause a midline vocal cord paralysis or something called a paramidline vocal cord paralysis. A midline vocal cord paralysis may allow good quality of voice (patients may not know their vocal cord is paralyzed) but their opening for breathing will be half of what it previously used to be. A paramidline (next to the midline (this is a floppy/ loose paralysis) vocal cord paralysis produces poor quality of voice (a hoarse and airy voice) but their breathing space between their vocal cords is less compromised. Paralysis of both recurrent laryngeal nerves is the most devastating injury to the voice box possible due to thyroid cancer surgery. Protect the nerves to your voice box by finding a truly expert thyroid cancer surgeon.
As a general rule, nerves do not like to be handled roughly. The nerves to the voice box should be handled with the most delicate and meticulous methods. The nerves to the voice box should be protected from any heat or mechanical injuries of every kind. I tend to explain to patients that nerves however are unpredictable. Even the most minimal safe identification of the nerve may produce transient weakness and sometimes the most extensive dissection (required) of a voice box nerve along its course may produce absolutely no change in vocal or breathing quality whatsoever. What is most important is that all of these nerves and their branches must be identified and managed with the utmost care. This is the art and expertise of thyroid cancer surgery. If these nerves are spared, even if they are temporarily dysfunctional following surgery, they will recover unless they have been irreversibly damaged. Not all, but almost all irreversible damage is caused by incompletely visualizing and inadvertently cutting a branch or branches of these nerves. Don’t let this happen to you. This is almost always due to inexperience of thyroid cancer surgeons. If a surgeon tells you that they will not identify the nerves during a thyroidectomy…..find another surgeon who tells you they always do. Nerve monitoring, a method of testing whether the voice box nerves can stimulate with a very small electrical current does not save nerves and does not prevent nerves from being damaged. What nerve monitoring can do is tell the surgeon if a nerve is damaged or at risk of note functioning following surgery. Nerve monitoring is not a substitute for excellent thyroid surgery.
The right recurrent laryngeal nerves path into the voice box is different from that of the left recurrent laryngeal nerve. Additionally, lymph nodes from thyroid cancer are commonly found underneath the right nerve to the voice box. In comparison, the thyroid cancer lymph nodes along the left nerve to the voice box are usually located to either side or in front of that nerve.
The recurrent laryngeal nerves, on either side, almost always produces multiple branches before they enter the voice box. All of these branches should be preserved whenever feasible. With only very rare exceptions, the only safe thyroid surgery identifies and spares all recurrent laryngeal nerve branches.
Only occurring on the right side of patients, a non-recurrent laryngeal nerve can be found. Here is a picture of just one such example.
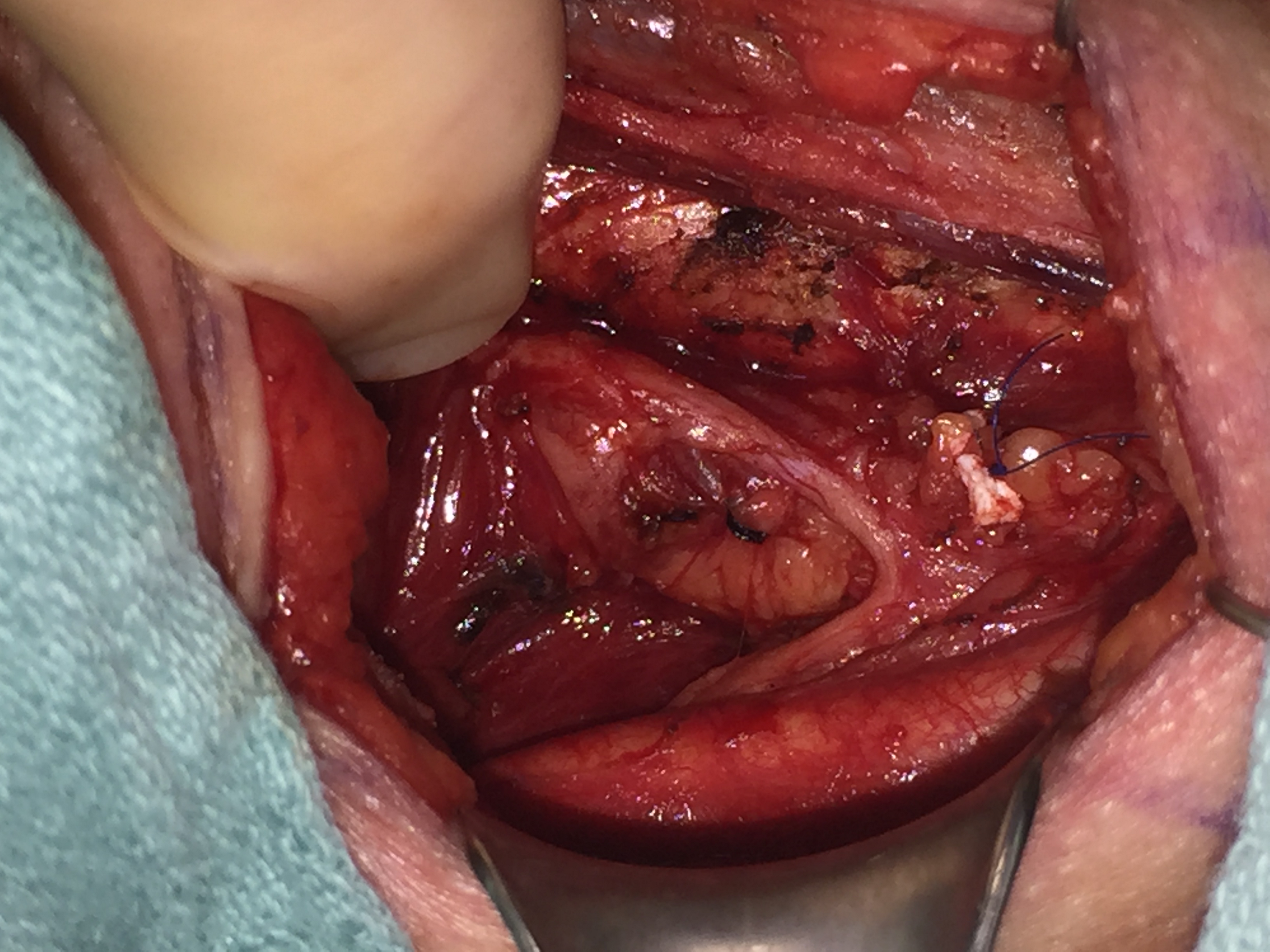
Non-recurrent laryngeal nerves are reported to be present in 1 in every 100 individuals. Non-recurrent laryngeal nerves are only present when an important artery of the upper chest passes behind the swallowing tube (esophagus) instead of its usual location (this is called a retroesophageal subclavian artery). Since I identify the recurrent laryngeal nerves at least six hundred times per year, I am confident that my experience has not found non-recurrent laryngeal nerves to be as frequent as reported. Nevertheless, identifying the voice box nerve, whether recurrent or non-recurrent is the only method to insure its safety in thyroid cancer surgery.
The external branch of the superior laryngeal nerve is located quite distinctly different from the recurrent laryngeal nerve. Its location may be very intimate with the blood vessels of the upper portion of the thyroid lobe called the superior thyroid artery and vein. As the upper portion of the thyroid (superior pole) is mobilized in thyroid surgery, this small branch or branches must be visualized and spared as well. This nerve controls tightening of the vocal cord as well as the feeling of the upper portion of the voice box.
What to read next
- Some more items go here
- How to become our patient