Understanding Tall Cell Variant of Papillary Thyroid Cancer

Introduction
Tall cell thyroid cancer is a variant of papillary thyroid cancer (PTC). Papillary thyroid cancer is by far the most common type of thyroid cancer, accounting for roughly 85% of cases. Until recently, thyroid cancer was the fastest growing cancer in the United States, mainly due to our ability to detect these cancers so well (Ultrasound, CT scan, MRI, etc.). Overall cure rate of all papillary thyroid cancer approaches 100%, for most patients, particularly in the hands of expert surgeons at specialized, high-volume thyroid centers. Tall cell thyroid cancer, however, can be more aggressive and challenging to deal with. Similar to classic PTC, tall cell variant outcomes and survival are directly tied to experience, expertise, and a complete understanding of the cancer (pathologic features, molecular/genetic profile, etc.) and treatment algorithm.
Understanding Tall Cell Variant of Papillary Thyroid Cancer
Below I will discuss what you need to know about tall cell thyroid cancer
Surgery is the mainstay of treatment
Thyroid surgery is the mainstay of treating all thyroid cancers. Tall cell thyroid cancer is no different. Even microscopic (less than 1 cm) tall cell thyroid cancers are clearly shown to have more unfavorable clinical features (lymph node metastasis, etc.) than classic microscopic papillary thyroid cancers and require surgery in all cases. There are 2 main types of thyroidectomy: thyroid lobectomy (removal of half of the thyroid) and total thyroidectomy (removal of the entire thyroid). Many tall cell thyroid cancers can be treated by removal of half the thyroid along with the lymph nodes that are located behind and around the thyroid. Numerous studies have shown that 20%- 30% of thyroid cancers have at least microscopic lymph node disease at the time of diagnosis and surgery. Expert evaluation and complete removal of all cancer with the first surgery are extremely important to avoid complications and leaving cancer behind.
In other instances, total thyroidectomy is needed to treat tall cell thyroid cancers that are large, have aggressive features [growth outside of the thyroid into surrounding tissue and structures (extrathyroidal extension), growth into tiny blood vessels in and around the cancer, lymphatic invasion] located in both halves of the thyroid, or when cancer has spread to lymph nodes in the neck. Again, removal of the lymph nodes behind and around the thyroid in the middle of the neck at a minimum is important to ensure the tall cell thyroid cancer is completely cured. Complete thyroid removal is riskier than thyroid surgery for half the thyroid. This is because both sides of the neck are worked on, exposing all 4 parathyroid glands (calcium control glands) as well as all the nerves to the voice box to potential damage. Thus, total thyroid removal should only be done by high-volume, experienced surgeons at busy centers such as ours.
Finally, tall cell thyroid cancer that has spread to lymph nodes in the side of the neck is treated by removing the whole thyroid (total thyroidectomy) along with lymph node dissection (neck dissection). This thyroid surgery is done for thyroid cancers that have spread to lymph nodes in the side of the neck (on the left, right, or both) or to the lymph nodes in the center of the neck around and behind the thyroid. Since tall cell thyroid cancer exhibits aggressive features more frequently and can be more resistant to radioactive iodine (RAI) treatment after surgery, skilled and expert surgery is imperative to improve cure rates and disease-free survival.
Tall cell thyroid cancer: The basics
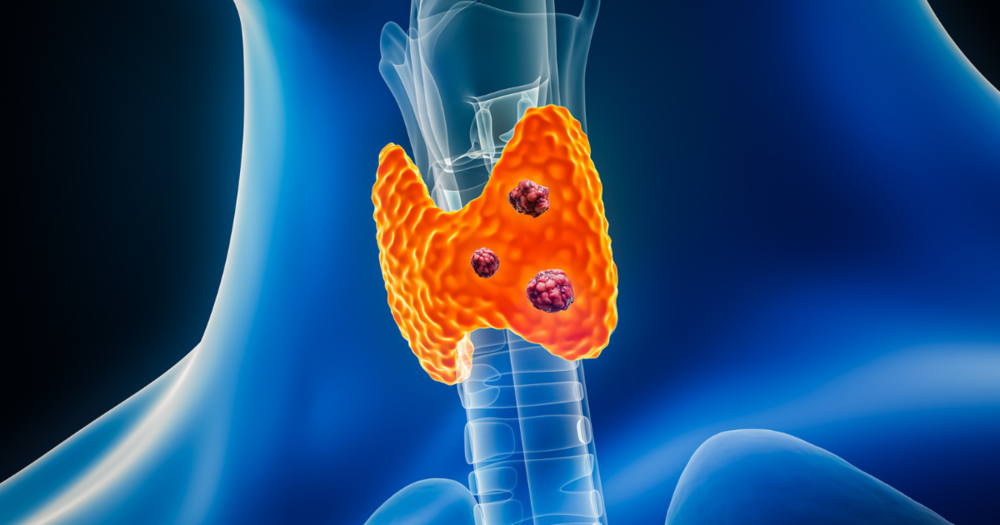
Tall cell thyroid cancer is a type or variant of papillary thyroid cancer. This was first recognized and described in 1976 as is reported to represent anywhere from 5%-19% of papillary thyroid cancers. Tall cell variant is classified by how the cancer cells look under a microscope when examined by the pathologist. Simply put, tall cell thyroid cancer is characterized by presence of ≥ 30% of tall cells (2 - 3 times taller than wide) and well developed papillary thyroid carcinoma nuclear features in the tumor cells.
Tall cell thyroid cancer tends to exhibit more aggressive features (i.e. extrathyroidal extension, growth into tiny blood vessels in and around the cancer, lymphatic invasion) than classic PTC and has historically purported to be more challenging to treat and cure. Additionally, tall cell variant of papillary thyroid cancer responds much less frequently to radioactive iodine treatment than classic papillary thyroid cancer. Often, but not always, tall cell thyroid cancer tends to present with a larger tumor, extrathyroidal extension, lymph node involvement, distant metastases, and at an older age when compared to classic PTC. In particular, cases where the cancer accumulates more than 1 molecular/genetic change (mutation) are clearly more fast-growing, aggressive, and difficult to cure than classic papillary thyroid cancer. When these tall cell thyroid cancer cells accumulate genetic mutations/changes, they are also more likely to turn into poorly-differentiated or anaplastic thyroid cancers that are exceptionally aggressive and difficult to cure. The aforementioned is likely due to numerous factors, but nevertheless, tall cell variant of PTC requires expert diagnosis, surgery, and follow-up at high-volume centers.
Not all tall cell thyroid cancer is created equal
Tall cell thyroid cancers tend to be more aggressive and difficult to cure, particularly when compared to standard or classic papillary thyroid cancer. Like most papillary thyroid cancers, they are rarely symptomatic and are not diagnosed with blood tests. Additionally, tall cell papillary microcarcinomas (cancers measuring less than 1 cm) are more likely to exhibit aggressive features or spread to lymph nodes than classic papillary microcarcinomas. The tall cell thyroid cancers that accumulate molecular/genetic changes can progress or turn into much more aggressive thyroid cancers as noted above.
Not all of these tall cell thyroid cancers, however, are bad or aggressive. Some behave and are cured just like most other papillary thyroid cancers, especially when diagnosed early. There are also instances where classic PTC has some tall cell features on pathology when examined under a microscope. Basically, a small percentage of cells have tall cell characteristics. Survival and risk in these scenarios are essentially the same when compared to classic PTC. In expert hands though, many of these cancers can be diagnosed and treated with surgery with similar outcomes to classic papillary thyroid cancer.
Tall cell thyroid cancer: Summary
Work-up and diagnosis of tall cell thyroid cancer begins with an expert high-resolution thyroid ultrasound and needle biopsy (FNA) if needed. This variant of papillary thyroid cancer is ultimately diagnosed after surgery when the cancer is examined under a microscope by the pathologist and 30% or more of the cells exhibit tall cell features. Tall cell thyroid cancer is treated with the correct surgery done at a very high-volume center, such as the Clayman Thyroid Center. These cancers, even when less than 1 cm, are generally more aggressive and difficulty to cure when compared to classic PTC. When diagnosed and treated in expert, experienced hands, outcomes and survival are excellent.

Our team of thyroid experts is here to help and guide you every step along the way during the diagnosis and surgery for your thyroid disease. The Clayman Thyroid Center is dedicated to providing world-class care for thyroid cancer and thyroid disease. To learn more and become a patient, please see our resources below.
Additional Resources
- Become our patient by filling out the form at this link.
- Learn more about The Clayman Thyroid Center here.
- Learn more about our sister surgeons at the Scarless Thyroid Surgery Center, Norman Parathyroid Center, and Carling Adrenal Center
- Learn more about the Hospital for Endocrine Surgery.